Motuel Julie, Biette Isaure, Srairi Mohamed, Mrozek Ségolène, Kurrek Matt M, Chaynes Patrick, Cognard Christophe, Fourcade Olivier, Geeraerts Thomas
Anesthesiology and Critical Care Department, Equipe d'accueil "Modélisation de l'agression tissulaire et nociceptive", University Hospital of Toulouse, University Toulouse 3 Paul Sabatier, Toulouse, France.
Neuroradiology Department, University Hospital of Toulouse, University Toulouse 3 Paul Sabatier, Toulouse, France.
Crit Care. 2014 Dec 9;18(6):676. doi: 10.1186/s13054-014-0676-9.
Brain midline shift (MLS) is a life-threatening condition that requires urgent diagnosis and treatment. We aimed to validate bedside assessment of MLS with Transcranial Sonography (TCS) in neurosurgical ICU patients by comparing it to CT.
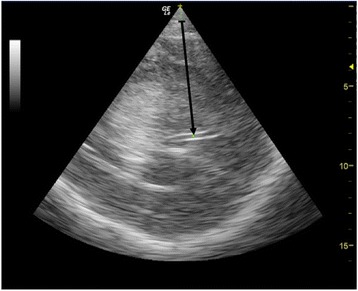
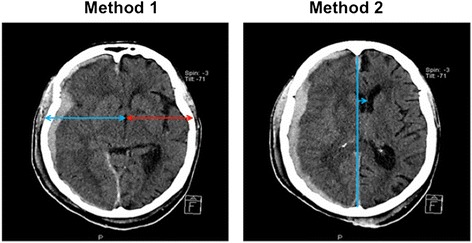
In this prospective single centre study, patients who underwent a head CT were included and a concomitant TCS performed. TCS MLS was determined by measuring the difference between the distance from skull to the third ventricle on both sides, using a 2 to 4 MHz probe through the temporal window. CT MLS was measured as the difference between the ideal midline and the septum pellucidum. A significant MLS was defined on head CT as > 0.5 cm.
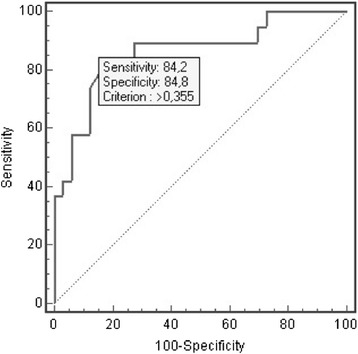
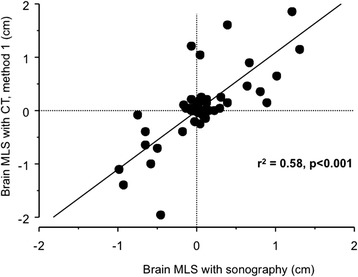
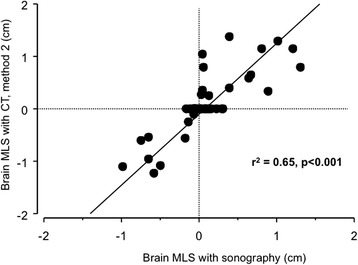
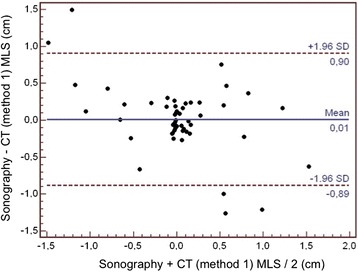
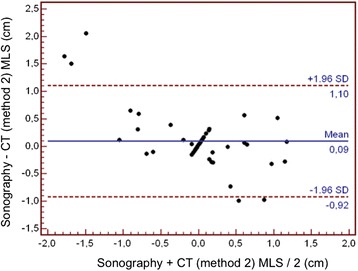
A total of 52 neurosurgical ICU patients were included. The MLS (mean ± SD) was 0.32 ± 0.36 cm using TCS and 0.47 ± 0.67 cm using CT. The Pearson's correlation coefficient (r(2)) between TCS and CT scan was 0.65 (P < 0.001). The bias was 0.09 cm and the limits of agreements were 1.10 and -0.92 cm. The area under the ROC curve for detecting a significant MLS with TCS was 0.86 (95% CI = 0.74 to 0.94), and, using 0.35 cm as a cut-off, the sensitivity was 84.2%, the specificity 84.8% and the positive likelihood ratio was 5.56.
This study suggests that TCS could detect MLS with reasonable accuracy in neurosurgical ICU patients and that it could serve as a bedside tool to facilitate early diagnosis and treatment for patients with a significant intracranial mass effect.
脑中线移位(MLS)是一种危及生命的状况,需要紧急诊断和治疗。我们旨在通过将经颅超声检查(TCS)与CT进行比较,验证神经外科重症监护病房(ICU)患者床边MLS评估的准确性。
在这项前瞻性单中心研究中,纳入接受头部CT检查的患者,并同时进行TCS检查。使用2至4MHz探头通过颞窗测量两侧颅骨至第三脑室距离的差值来确定TCS MLS。CT MLS测量为理想中线与透明隔之间的差值。头部CT上显著MLS定义为>0.5cm。
共纳入52例神经外科ICU患者。TCS测量的MLS(均值±标准差)为0.32±0.36cm,CT测量的为0.47±0.67cm。TCS与CT扫描之间的Pearson相关系数(r(2))为0.65(P<0.001)。偏差为0.09cm,一致性界限为1.10和-0.92cm。TCS检测显著MLS的ROC曲线下面积为0.86(95%CI=0.74至0.94),以0.35cm为临界值时,敏感性为84.2%,特异性为84.8%,阳性似然比为5.56。
本研究表明,TCS能够在神经外科ICU患者中以合理的准确性检测MLS,并且可作为一种床边工具,便于对有显著颅内占位效应的患者进行早期诊断和治疗。