Department of Paediatrics, University of Pretoria, Pretoria, South Africa.
BMC Public Health. 2014 Dec 13;14:1265. doi: 10.1186/1471-2458-14-1265.
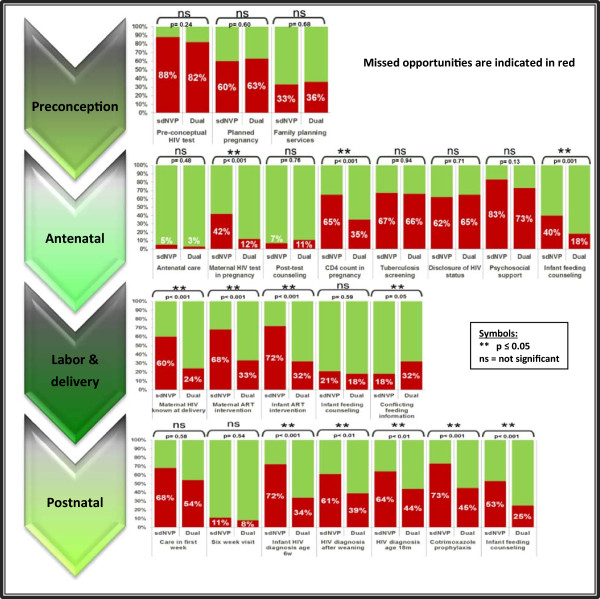
The prevention of mother-to-child transmission (PMTCT) program in South Africa is now successful in ensuring HIV-free survival for most HIV-exposed children, but gaps in PMTCT coverage remain. The study objective was to identify missed opportunities for prevention of mother-to-child transmission of HIV using the four PMTCT stages outlined in National Guidelines.
This descriptive study enrolled HIV-exposed children who were below the age of 7 years and therefore born during the South African PMTCT era. The study site was in Gauteng, South Africa and enrolment was from June 2009 to May 2010. The clinical history was obtained through a structured caregiver interview and review of medical records and included socio-demographic data, medical history, HIV interventions, infant feeding information and HIV results. The study group was divided into the "single dose nevirapine" ("sdNVP") and "dual-therapy" (nevirapine & zidovudine) groups due to PMTCT program change in February 2008, with subsequent comparison between the groups regarding PMTCT steps during the preconception stage, antenatal care, labor and delivery and postpartum care.
Two-hundred-and-one HIV-exposed children were enrolled: 137 (68%) children were HIV infected and 64 (32%) were HIV uninfected. All children were born between 2002 and 2009, with 78 (39%) in the "sdNVP" and 123 (61%) in the "dual-therapy" groups. The results demonstrate significant improvements in antenatal HIV testing and PMTCT enrolment, known maternal HIV diagnosis at delivery, mother-infant antiretroviral interventions, infant HIV-diagnosis and cotrimoxazole prophylaxis. Missed opportunities without improvement include pre-conceptual HIV-services and family planning, tuberculosis screening, HIV disclosure, psychosocial support and postnatal care. Not receiving consistent infant feeding messaging was the only PMTCT component that worsened over time.
Multiple missed opportunities for optimal PMTCT were identified, which collectively increase children's risk of HIV acquisition. Although HIV-testing and antiretroviral interventions improved, all PMTCT components need to be optimized to reach the goal of total pediatric HIV elimination.
南非的母婴传播预防(PMTCT)项目如今已成功确保大多数艾滋病毒暴露儿童的 HIV 检测呈阴性,但是 PMTCT 覆盖率仍存在差距。本研究的目的是利用国家指南中概述的四个 PMTCT 阶段,确定母婴传播 HIV 的预防措施中存在的疏漏。
本描述性研究纳入了年龄小于 7 岁的 HIV 暴露儿童,这些儿童出生于南非的 PMTCT 时代。研究地点在南非豪登省,招募时间为 2009 年 6 月至 2010 年 5 月。临床病史通过结构化的照顾者访谈和病历回顾获得,包括社会人口统计学数据、病史、HIV 干预措施、婴儿喂养信息和 HIV 结果。由于 2008 年 2 月 PMTCT 项目发生变化,该研究组被分为“单剂量奈韦拉平(sdNVP)”和“双疗法(奈韦拉平+齐多夫定)”组,随后对两组在孕前阶段、产前保健、分娩和产后护理期间的 PMTCT 步骤进行了比较。
共纳入 211 名 HIV 暴露儿童:137 名(68%)儿童感染 HIV,64 名(32%)儿童未感染 HIV。所有儿童均出生于 2002 年至 2009 年之间,其中 78 名(39%)在“sdNVP”组,123 名(61%)在“双疗法”组。结果表明,产前 HIV 检测和 PMTCT 参与率、已知产妇 HIV 诊断、母婴抗逆转录病毒干预、婴儿 HIV 诊断和复方磺胺甲噁唑预防都有显著提高。未改善的疏漏包括孕前 HIV 服务和计划生育、结核病筛查、HIV 披露、心理社会支持和产后护理。没有持续提供一致的婴儿喂养信息是唯一随着时间推移而恶化的 PMTCT 组成部分。
确定了多个错失的最佳 PMTCT 机会,这些机会共同增加了儿童获得 HIV 的风险。尽管 HIV 检测和抗逆转录病毒干预措施有所改善,但所有 PMTCT 组成部分都需要优化,以实现儿童 HIV 消除的目标。