Division of Infectious Diseases, Massachusetts General Hospital, Boston, Massachusetts, United States of America.
PLoS One. 2011;6(6):e20224. doi: 10.1371/journal.pone.0020224. Epub 2011 Jun 2.
The Zimbabwean national prevention of mother-to-child HIV transmission (PMTCT) program provided primarily single-dose nevirapine (sdNVP) from 2002-2009 and is currently replacing sdNVP with more effective antiretroviral (ARV) regimens.
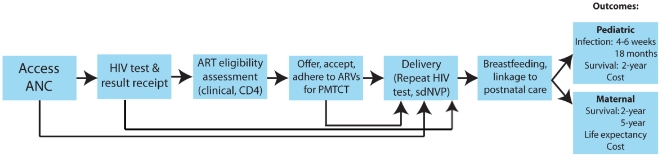
Published HIV and PMTCT models, with local trial and programmatic data, were used to simulate a cohort of HIV-infected, pregnant/breastfeeding women in Zimbabwe (mean age 24.0 years, mean CD4 451 cells/µL). We compared five PMTCT regimens at a fixed level of PMTCT medication uptake: 1) no antenatal ARVs (comparator); 2) sdNVP; 3) WHO 2010 guidelines using "Option A" (zidovudine during pregnancy/infant NVP during breastfeeding for women without advanced HIV disease; lifelong 3-drug antiretroviral therapy (ART) for women with advanced disease); 4) WHO "Option B" (ART during pregnancy/breastfeeding without advanced disease; lifelong ART with advanced disease); and 5) "Option B+:" lifelong ART for all pregnant/breastfeeding, HIV-infected women. Pediatric (4-6 week and 18-month infection risk, 2-year survival) and maternal (2- and 5-year survival, life expectancy from delivery) outcomes were projected.
Eighteen-month pediatric infection risks ranged from 25.8% (no antenatal ARVs) to 10.9% (Options B/B+). Although maternal short-term outcomes (2- and 5-year survival) varied only slightly by regimen, maternal life expectancy was reduced after receipt of sdNVP (13.8 years) or Option B (13.9 years) compared to no antenatal ARVs (14.0 years), Option A (14.0 years), or Option B+ (14.5 years).
Replacement of sdNVP with currently recommended regimens for PMTCT (WHO Options A, B, or B+) is necessary to reduce infant HIV infection risk in Zimbabwe. The planned transition to Option A may also improve both pediatric and maternal outcomes.
津巴布韦国家预防母婴传播艾滋病毒(PMTCT)计划从 2002 年至 2009 年主要提供单剂量奈韦拉平(sdNVP),目前正在用更有效的抗逆转录病毒(ARV)方案替代 sdNVP。
使用已发表的 HIV 和 PMTCT 模型以及当地试验和项目数据,模拟津巴布韦一组感染艾滋病毒的孕妇/哺乳期妇女(平均年龄 24.0 岁,平均 CD4 细胞 451 个/µL)。我们比较了在固定的 PMTCT 药物使用率下的五种 PMTCT 方案:1)不使用产前 ARV(对照);2)sdNVP;3)世卫组织 2010 年指南采用“选项 A”(无晚期 HIV 疾病的孕妇使用齐多夫定/婴儿在哺乳期使用 NVP;晚期疾病的妇女终生三药抗逆转录病毒治疗(ART));4)世卫组织“选项 B”(无晚期疾病的孕妇/哺乳期妇女使用 ART;晚期疾病的妇女终生使用 ART);5)“选项 B+”:所有孕妇/哺乳期 HIV 感染妇女终生使用 ART。预测了儿科(4-6 周和 18 个月的感染风险、2 年生存率)和产妇(2 年和 5 年生存率、分娩时的预期寿命)结局。
18 个月的儿科感染风险范围从无产前 ARV 的 25.8%到“选项 B+”的 10.9%。尽管方案之间产妇短期结局(2 年和 5 年生存率)略有不同,但与无产前 ARV(14.0 年)、“选项 A”(14.0 年)或“选项 B+”(14.5 年)相比,接受 sdNVP 或“选项 B”(13.9 年)后,产妇的预期寿命会降低。
为了降低津巴布韦婴儿的 HIV 感染风险,有必要用目前推荐的 PMTCT 方案(世卫组织“选项 A”、“选项 B”或“选项 B+”)替代 sdNVP。计划过渡到“选项 A”也可能改善儿科和产妇的结局。