Kron Irving L, Hung Judy, Overbey Jessica R, Bouchard Denis, Gelijns Annetine C, Moskowitz Alan J, Voisine Pierre, O'Gara Patrick T, Argenziano Michael, Michler Robert E, Gillinov Marc, Puskas John D, Gammie James S, Mack Michael J, Smith Peter K, Sai-Sudhakar Chittoor, Gardner Timothy J, Ailawadi Gorav, Zeng Xin, O'Sullivan Karen, Parides Michael K, Swayze Roger, Thourani Vinod, Rose Eric A, Perrault Louis P, Acker Michael A
Division of Thoracic and Cardiovascular Surgery, University of Virginia School of Medicine, Charlottesville, Va.
Division of Cardiology, Massachusetts General Hospital, Boston, Mass.
J Thorac Cardiovasc Surg. 2015 Mar;149(3):752-61.e1. doi: 10.1016/j.jtcvs.2014.10.120. Epub 2014 Nov 6.
The Cardiothoracic Surgical Trials Network recently reported no difference in the primary end point of left ventricular end-systolic volume index at 1 year postsurgery in patients randomized to repair (n = 126) or replacement (n = 125) for severe ischemic mitral regurgitation. However, patients undergoing repair experienced significantly more recurrent mitral regurgitation than patients undergoing replacement (32.6% vs 2.3%). We examined whether baseline echocardiographic and clinical characteristics could identify those who will develop moderate/severe recurrent mitral regurgitation or die.
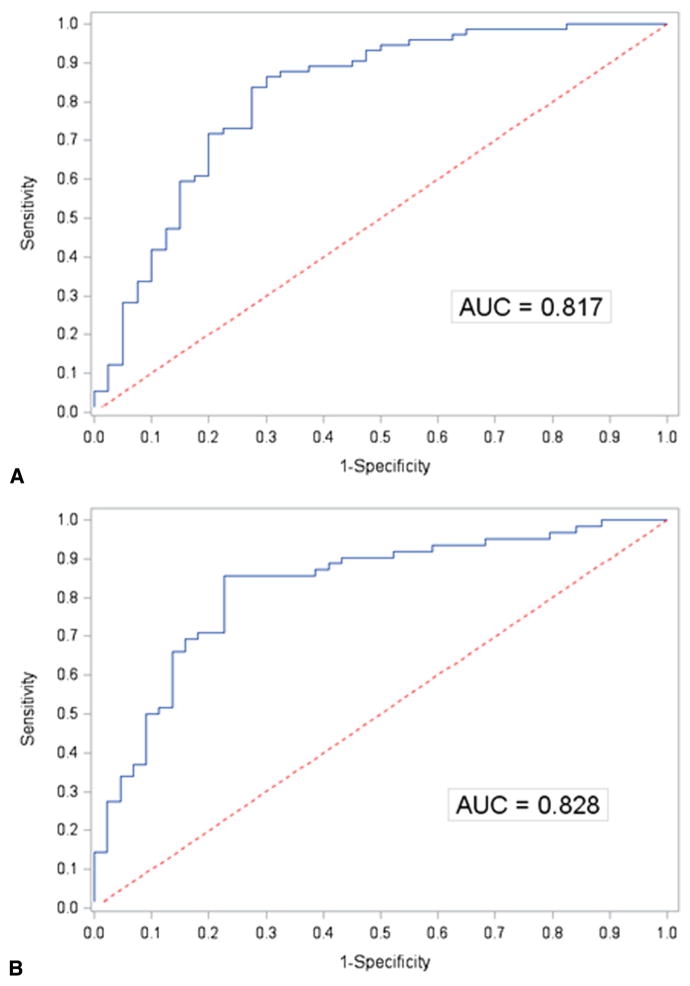
Our analysis includes 116 patients who were randomized to and received mitral valve repair. Logistic regression was used to estimate a model-based probability of recurrence or death from baseline factors. Receiver operating characteristic curves were constructed from these estimated probabilities to determine classification cut-points maximizing accuracy of prediction based on sensitivity and specificity.
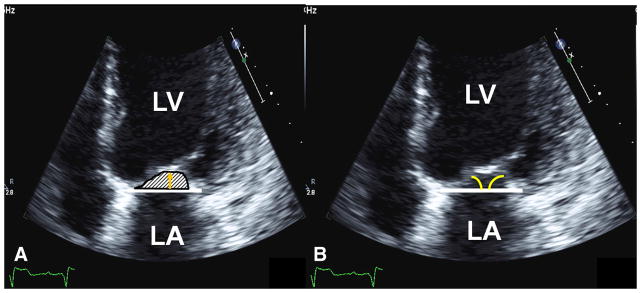
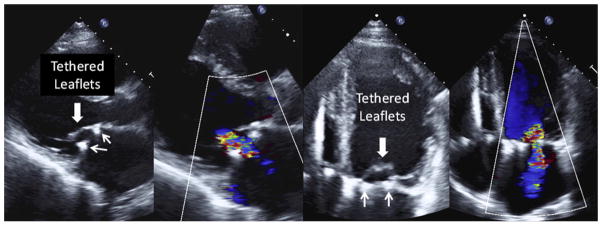
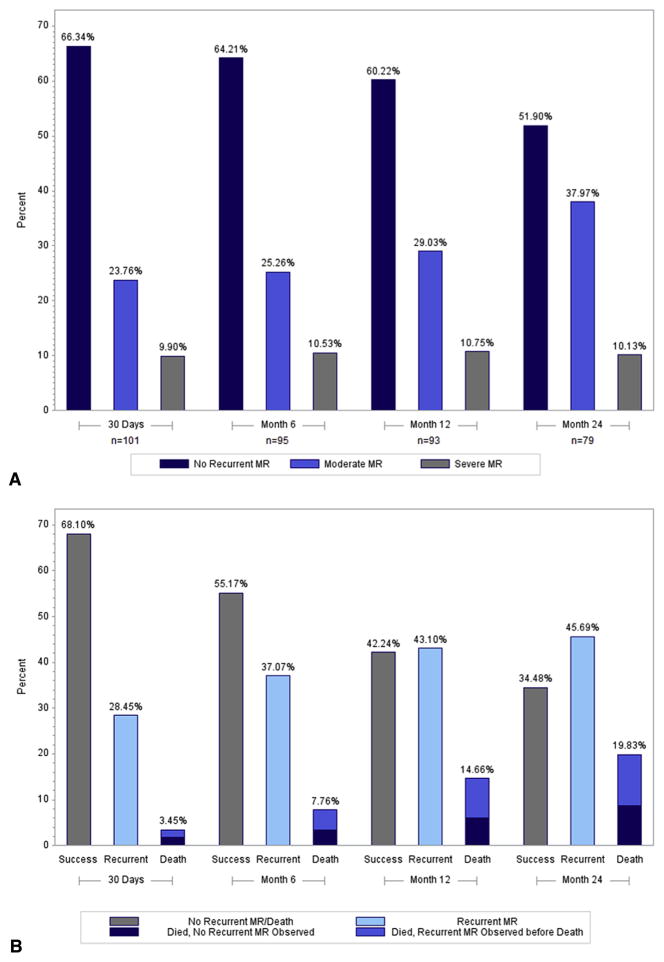
Of the 116 patients, 6 received a replacement before leaving the operating room; all other patients had mild or less mitral regurgitation on intraoperative echocardiogram after repair. During the 2-year follow-up period, 76 patients developed moderate/severe mitral regurgitation or died (53 mitral regurgitation recurrences, 13 mitral regurgitation recurrences and death, and 10 deaths). The mechanism for recurrent mitral regurgitation was largely mitral valve leaflet tethering. Our model (including age, body mass index, sex, race, effective regurgitant orifice area, basal aneurysm/dyskinesis, New York Heart Association class, history of coronary artery bypass grafting, percutaneous coronary intervention, or ventricular arrhythmias) yielded an area under the receiver operating characteristic curve of 0.82.
The model demonstrated good discrimination in identifying patients who will survive 2 years without recurrent mitral regurgitation after mitral valve repair. Although our results require validation, they offer a clinically relevant risk score for selection of surgical candidates for this procedure.
心胸外科试验网络最近报告称,在因严重缺血性二尖瓣反流而随机接受修复术(n = 126)或置换术(n = 125)的患者中,术后1年左心室收缩末期容积指数的主要终点无差异。然而,接受修复术的患者二尖瓣反流复发明显多于接受置换术的患者(32.6%对2.3%)。我们研究了基线超声心动图和临床特征是否能识别出那些会发生中/重度二尖瓣反流复发或死亡的患者。
我们的分析纳入了116例随机接受二尖瓣修复术并接受该手术的患者。使用逻辑回归从基线因素估计复发或死亡的基于模型的概率。根据这些估计概率构建受试者工作特征曲线,以确定基于敏感性和特异性最大化预测准确性的分类切点。
116例患者中,6例在离开手术室前接受了置换术;所有其他患者在修复术后的术中超声心动图显示二尖瓣反流为轻度或更低程度。在2年随访期内,76例患者发生中/重度二尖瓣反流或死亡(53例二尖瓣反流复发,13例二尖瓣反流复发并死亡,10例死亡)。二尖瓣反流复发的机制主要是二尖瓣叶束缚。我们的模型(包括年龄、体重指数、性别、种族、有效反流口面积、基底动脉瘤/运动障碍、纽约心脏协会分级、冠状动脉搭桥术史、经皮冠状动脉介入治疗或室性心律失常)在受试者工作特征曲线下的面积为0.82。
该模型在识别二尖瓣修复术后2年无二尖瓣反流复发存活患者方面具有良好的辨别能力。尽管我们的结果需要验证,但它们为该手术的手术候选人选择提供了一个临床相关的风险评分。