Kang Jeonghyun, Lee Hak Woo, Kim Im-kyung, Kim Nam Kyu, Sohn Seung-Kook, Lee Kang Young
Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
Yonsei Med J. 2015 Jan;56(1):175-81. doi: 10.3349/ymj.2015.56.1.175.
The estimation of regional lymph node metastasis (LNM) risk in T1 colorectal cancer is based on histologic examination and imaging of the primary tumor. High-frequency microsatellite instability (MSI-H) is likely to decrease the possibility of metastasis to either regional lymph nodes or distant organs in colorectal cancers. This study evaluated the clinical implications of MSI in T1 colorectal cancer with emphasis on the usefulness of MSI as a predictive factor for regional LNM.
A total of 133 patients who underwent radical resection for T1 colorectal cancer were included. Genomic DNA was extracted from normal and tumor tissues and amplified by polymerase chain reaction (PCR). Five microsatellite markers, BAT-25, BAT-26, D2S123, D5S346, and D17S250, were used. MSI and clinicopathological parameters were evaluated as potential predictors of LNM using univariate and multivariate analyses.
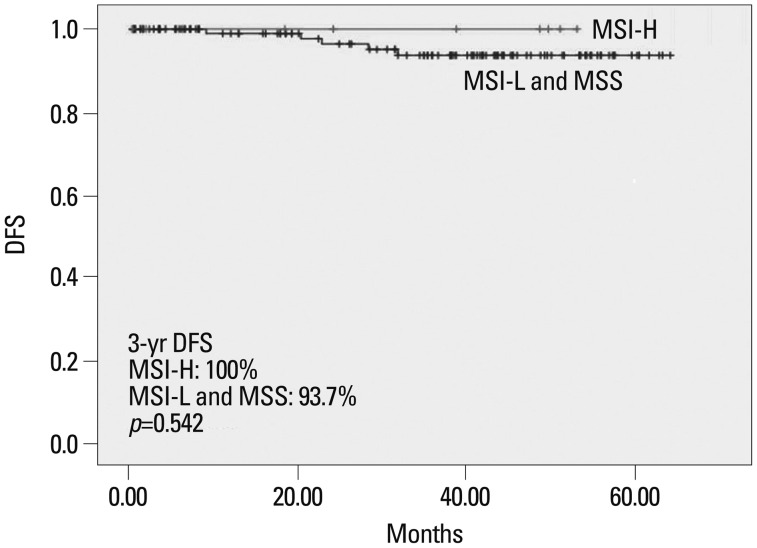
Among 133 T1 colorectal cancer patients, MSI-H, low-frequency microsatellite instability (MSI-L), and microsatellite stable (MSS) colorectal cancers accounted for 7.5%, 6%, and 86.5%, respectively. MSI-H tumors showed a female predominance, a proximal location and more retrieved lymph nodes. Twenty-two patients (16.5%) had regional LNM. Lymphovascular invasion and depth of invasion were significantly associated with LNM. There was no LNM in 10 MSI-H patients; however, MSI status was not significantly correlated with LNM. Disease-free survival did not differ between patients with MSI-H and those with MSI-L/MSS.
MSI status could serve as a negative predictive factor in estimating LNM in T1 colorectal cancer, given that LNM was not detected in MSI-H patients. However, validation of our result in a different cohort is necessary.
T1期结直肠癌区域淋巴结转移(LNM)风险的评估基于原发肿瘤的组织学检查和影像学检查。高频微卫星不稳定性(MSI-H)可能会降低结直肠癌转移至区域淋巴结或远处器官的可能性。本研究评估了MSI在T1期结直肠癌中的临床意义,重点关注MSI作为区域LNM预测因子的实用性。
纳入133例行T1期结直肠癌根治性切除术的患者。从正常组织和肿瘤组织中提取基因组DNA,并通过聚合酶链反应(PCR)进行扩增。使用五个微卫星标记物,即BAT-25、BAT-26、D2S123、D5S346和D17S250。采用单因素和多因素分析评估MSI和临床病理参数作为LNM的潜在预测因子。
在133例T1期结直肠癌患者中,MSI-H、低频微卫星不稳定性(MSI-L)和微卫星稳定(MSS)的结直肠癌分别占7.5%、6%和86.5%。MSI-H肿瘤以女性居多,位于近端且回收的淋巴结更多。22例患者(16.5%)发生区域LNM。淋巴管浸润和浸润深度与LNM显著相关。10例MSI-H患者未发生LNM;然而,MSI状态与LNM无显著相关性。MSI-H患者与MSI-L/MSS患者的无病生存期无差异。
鉴于MSI-H患者未检测到LNM,MSI状态可作为T1期结直肠癌LNM评估的阴性预测因子。然而,需要在不同队列中验证我们的结果。