Human Cellular Therapy Laboratory, Division of Transfusion Medicine, Department of Laboratory Medicine and Pathology, Mayo Clinic, 200 First Street, Rochester, MN, USA.
Division of Hematology, Department of Medicine, Mayo Clinic, 200 First Street, Rochester, MN, USA.
J Immunother Cancer. 2013 Jun 27;1:7. doi: 10.1186/2051-1426-1-7. eCollection 2013.
We have developed a novel approach to categorize immunity in patients that uses a combination of whole blood flow cytometry and hierarchical clustering.
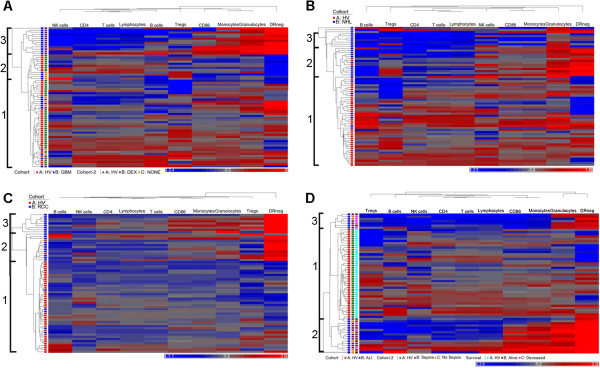
Our approach was based on determining the number (cells/μl) of the major leukocyte subsets in unfractionated, whole blood using quantitative flow cytometry. These measurements were performed in 40 healthy volunteers and 120 patients with glioblastoma, renal cell carcinoma, non-Hodgkin lymphoma, ovarian cancer or acute lung injury. After normalization, we used unsupervised hierarchical clustering to sort individuals by similarity into discreet groups we call immune profiles.
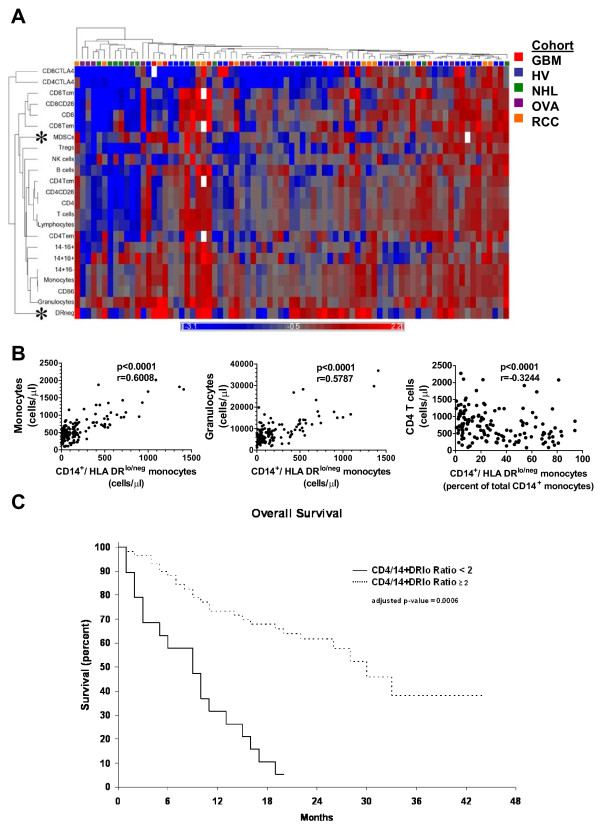
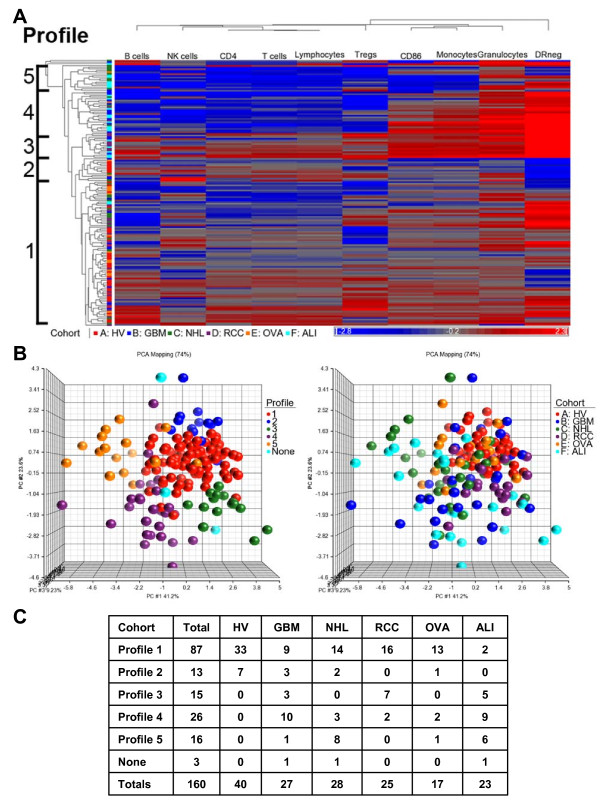
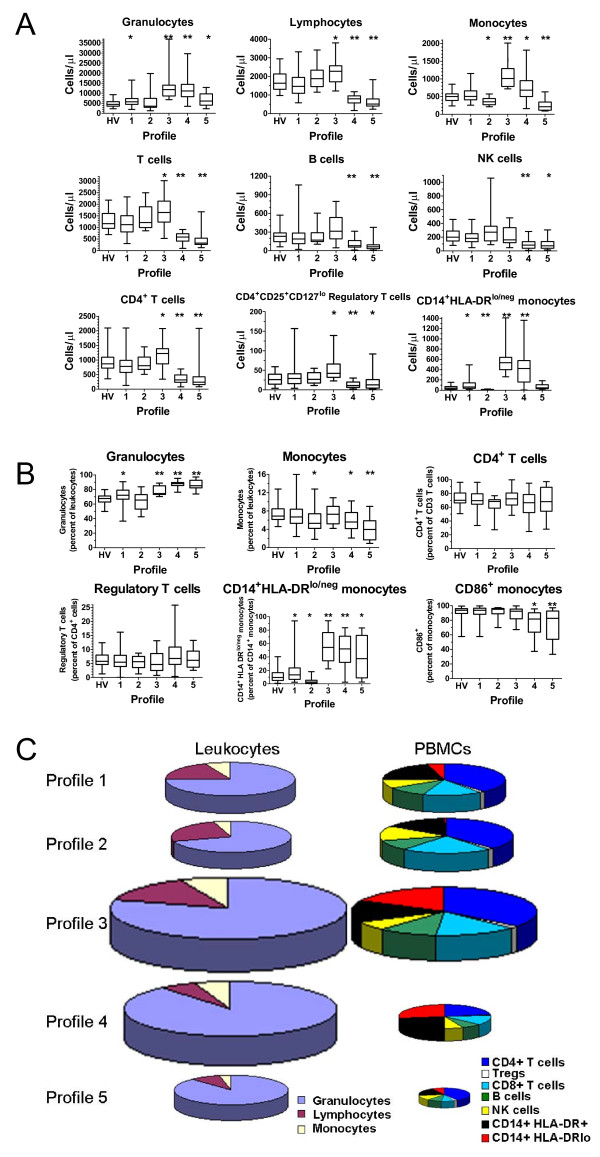
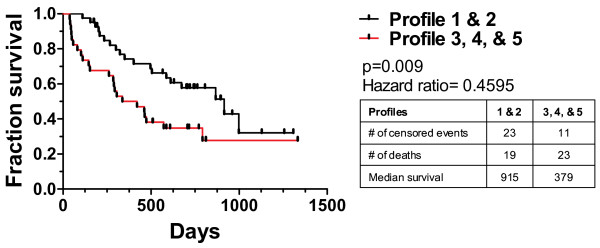
Five immune profiles were identified. Four of the diseases tested had patients distributed across at least four of the profiles. Cancer patients found in immune profiles dominated by healthy volunteers showed improved survival (p < 0.01). Clustering objectively identified relationships between immune markers. We found a positive correlation between the number of granulocytes and immunosuppressive CD14(+)HLA-DR(lo/neg) monocytes and no correlation between CD14(+)HLA-DR(lo/neg) monocytes and Lin(-)CD33(+)HLA-DR(-) myeloid derived suppressor cells. Clustering analysis identified a potential biomarker predictive of survival across cancer types consisting of the ratio of CD4(+) T cells/μl to CD14(+)HLA-DR(lo/neg) monocytes/μL of blood.
Comprehensive multi-factorial immune analysis resulting in immune profiles were prognostic, uncovered relationships among immune markers and identified a potential biomarker for the prognosis of cancer. Immune profiles may be useful to streamline evaluation of immune modulating therapies and continue to identify immune based biomarkers.
我们开发了一种新的方法来对患者的免疫进行分类,该方法结合了全血流式细胞术和层次聚类。
我们的方法基于使用定量流式细胞术确定未分馏全血中主要白细胞亚群的数量(细胞/μl)。在 40 名健康志愿者和 120 名患有胶质母细胞瘤、肾细胞癌、非霍奇金淋巴瘤、卵巢癌或急性肺损伤的患者中进行了这些测量。归一化后,我们使用无监督层次聚类根据相似性将个体分类为离散组,我们称之为免疫谱。
确定了五种免疫谱。四种测试疾病的患者分布在至少四种免疫谱中。在以健康志愿者为主的免疫谱中发现的癌症患者的生存率提高(p<0.01)。聚类客观地识别了免疫标志物之间的关系。我们发现粒细胞数量与免疫抑制性 CD14(+)HLA-DR(lo/neg)单核细胞呈正相关,而 CD14(+)HLA-DR(lo/neg)单核细胞与 Lin(-)CD33(+)HLA-DR(-)髓系来源抑制细胞之间无相关性。聚类分析确定了一个潜在的预测癌症各类型生存率的生物标志物,由 CD4(+)T 细胞/μl 与 CD14(+)HLA-DR(lo/neg)单核细胞/μl 的比值组成。
综合多因素免疫分析产生的免疫谱具有预后意义,揭示了免疫标志物之间的关系,并确定了癌症预后的潜在生物标志物。免疫谱可能有助于简化免疫调节治疗的评估,并继续识别基于免疫的生物标志物。