Department of Healthcare Economics and Quality Management, Graduate School of Medicine, Kyoto University, Yoshida Konoe-cho, Sakyo-ku, Kyoto City, Kyoto 606-8501, Japan.
BMC Pulm Med. 2014 Dec 16;14:203. doi: 10.1186/1471-2466-14-203.
Community-acquired pneumonia (CAP) is a common cause of patient hospitalization and death, and its burden on the healthcare system is increasing in aging societies. Here, we develop and internally validate risk-adjustment models and scoring systems for predicting mortality in CAP patients to enable more precise measurements of hospital performance.
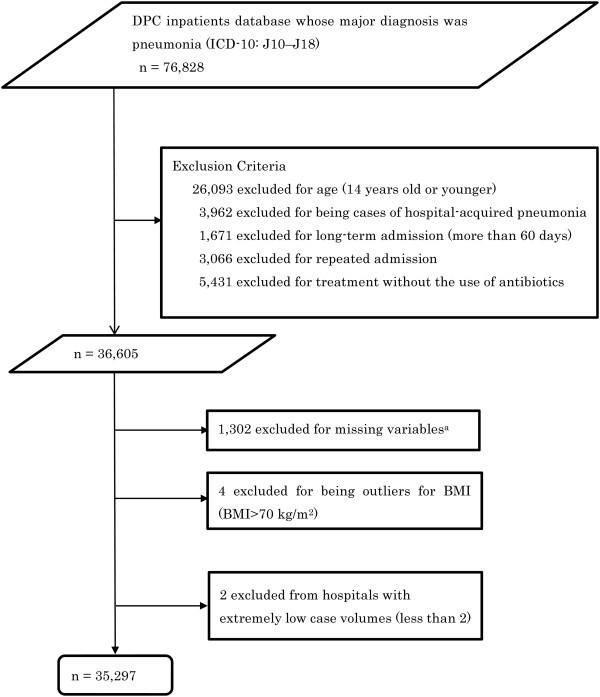
Using a multicenter administrative claims database, we analyzed 35,297 patients hospitalized for CAP who had been discharged between April 1, 2012 and September 30, 2013 from 303 acute care hospitals in Japan. We developed hierarchical logistic regression models to analyze predictors of in-hospital mortality, and validated the models using the bootstrap method. Discrimination of the models was assessed using c-statistics. Additionally, we developed scoring systems based on predictors identified in the regression models.
The 30-day in-hospital mortality rate was 5.8%. Predictors of in-hospital mortality included advanced age, high blood urea nitrogen level or dehydration, orientation disturbance, respiratory failure, low blood pressure, high C-reactive protein levels or high degree of pneumonic infiltration, cancer, and use of mechanical ventilation or vasopressors. Our models showed high levels of discrimination for mortality prediction, with a c-statistic of 0.89 (95% confidence interval: 0.89-0.90) in the bootstrap-corrected model. The scoring system based on 8 selected variables also showed good discrimination, with a c-statistic of 0.87 (95% confidence interval: 0.86-0.88).
Our mortality prediction models using administrative data showed good discriminatory power in CAP patients. These risk-adjustment models may support improvements in quality of care through accurate hospital evaluations and inter-hospital comparisons.
社区获得性肺炎(CAP)是导致患者住院和死亡的常见原因,在老龄化社会中,其给医疗系统带来的负担日益加重。在此,我们开发并内部验证了用于预测 CAP 患者死亡率的风险调整模型和评分系统,以更精确地衡量医院绩效。
我们使用多中心行政索赔数据库,分析了 2012 年 4 月 1 日至 2013 年 9 月 30 日期间从日本 303 家急性护理医院出院的 35297 例 CAP 住院患者。我们建立了分层逻辑回归模型来分析住院死亡率的预测因素,并使用自举法验证模型。使用 C 统计量评估模型的区分能力。此外,我们还基于回归模型中确定的预测因素开发了评分系统。
30 天住院死亡率为 5.8%。住院死亡率的预测因素包括高龄、高血尿素氮或脱水、定向障碍、呼吸衰竭、低血压、高 C 反应蛋白水平或高肺炎浸润程度、癌症以及使用机械通气或血管加压素。我们的模型对死亡率预测具有较高的区分能力,自举校正模型的 C 统计量为 0.89(95%置信区间:0.89-0.90)。基于 8 个选定变量的评分系统也具有良好的区分能力,C 统计量为 0.87(95%置信区间:0.86-0.88)。
我们使用行政数据的死亡率预测模型在 CAP 患者中具有良好的区分能力。这些风险调整模型可以通过准确的医院评估和医院间比较来支持改善护理质量。