Pullar Nadine Durema, Steinum Harald, Bruun Johan Nikolai, Dyrhol-Riise Anne Ma
Department of Internal Medicine, Section for Infectious Diseases, University Hospital of Northern Norway, N-9038, Tromsø, Norway.
Department of Clinical Medicine, Faculty of Health Sciences, University of Tromsø, N-9037, Tromsø, Norway.
BMC Infect Dis. 2014 Dec 17;14:667. doi: 10.1186/s12879-014-0667-0.
Interferon-γ release assays (IGRA) serve as immunodiagnostics of tuberculosis (TB) infection to identify individuals with latent TB infection (LTBI) eligible for preventive anti-TB therapy. In this longitudinal study of HIV-infected LTBI patients we have observed for possible progression to active TB as well as evaluated repeated IGRA testing in a TB low-endemic setting.
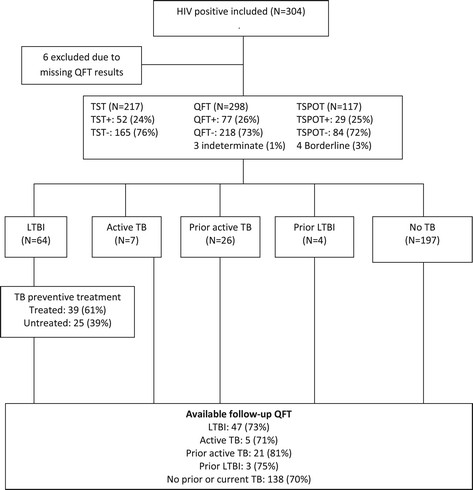
QuantiFERON TB-Gold In-tube® assay (QFT), TB-SPOT.TB® (TSPOT) and tuberculin skin test (TST) were performed on 298 HIV-patients recruited from seven out-patient clinics in Norway. Patients with active TB, LTBI and negative IGRA were followed with repeat QFTs and clinical evaluation over a period of 24 months.
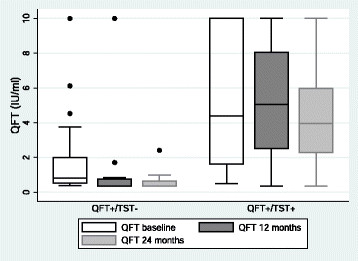
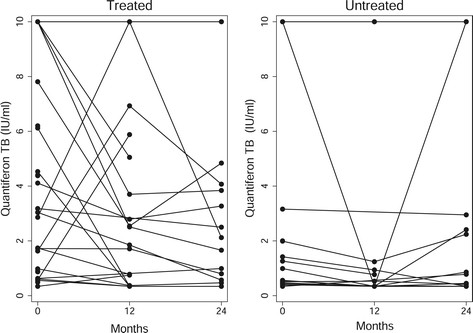
Seven HIV-patients (median CD4 count 270; IQR 50-340) were diagnosed with active TB at inclusion, all IGRA positive. Sixty-four (21%) HIV-patients (median CD4 count 471; IQR 342-638) were diagnosed with LTBI and of these 39 (61%) received TB preventive treatment. Neither treated nor untreated HIV-infected LTBI patients developed active TB during the 24 months. At baseline, the median interferon-γ (INF-γ) level measured by QFT was 3.48 IU/ml (IQR 0.94-8.91 IU/ml) for treated LTBI compared to 1.13 IU/ml (IQR 0.47-4.25 IU/ml) for untreated LTBI patients (p = 0.029). The QFT reversion rates were 75% for active TB, 23% for treated LTBI and 44% for untreated LTBI, whereas the conversion rate for the non-TB group was 7% despite no new TB exposure. There was no significant difference in the trend of INF-γ levels over time between treated and untreated LTBI patients.
The prevalence of LTBI is high among HIV-patients, but the risk of developing active TB seems to be low in patients with high CD4 counts in this TB low-endemic setting. In several patients, especially with baseline IFN-γ levels close to cut-offs, the QFT tests reverted to negative independent of preventive anti-TB treatment indicating possibly false positive tests. This highlights the importance of defining reliable cut-offs for immunodiagnostic tests and deferring preventive therapy in selected patients. Randomized studies with longer follow-up time are needed to identify HIV-patients that would benefit from LTBI treatment in a TB low-endemic setting.
干扰素-γ释放试验(IGRA)用作结核病(TB)感染的免疫诊断方法,以识别有资格接受预防性抗结核治疗的潜伏性结核感染(LTBI)个体。在这项针对HIV感染的LTBI患者的纵向研究中,我们观察了其进展为活动性结核病的可能性,并在结核病低流行地区评估了重复IGRA检测。
对从挪威7家门诊招募的298例HIV患者进行了全血γ-干扰素释放试验(QFT)、结核感染T细胞检测(TSPOT)和结核菌素皮肤试验(TST)。对活动性结核病、LTBI和IGRA阴性的患者进行为期24个月的重复QFT检测和临床评估。
7例HIV患者(CD4细胞计数中位数为270;四分位间距为50 - 340)在纳入研究时被诊断为活动性结核病,所有IGRA检测均为阳性。64例(21%)HIV患者(CD4细胞计数中位数为471;四分位间距为342 - 638)被诊断为LTBI,其中有39例(61%)接受了结核预防性治疗。在这24个月期间,接受治疗和未接受治疗的HIV感染LTBI患者均未发展为活动性结核病。基线时,接受治疗的LTBI患者通过QFT检测测得的干扰素-γ(INF-γ)水平中位数为3.48 IU/ml(四分位间距为0.94 - 8.91 IU/ml),而未接受治疗的LTBI患者为1.13 IU/ml(四分位间距为0.47 - 4.25 IU/ml)(p = 0.029)。活动性结核病患者的QFT逆转率为75%,接受治疗的LTBI患者为23%,未接受治疗的LTBI患者为44%,而非结核病组的转化率为7%,尽管没有新的结核暴露。接受治疗和未接受治疗的LTBI患者之间,INF-γ水平随时间变化的趋势没有显著差异。
在HIV患者中LTBI的患病率较高,但在这个结核病低流行地区,CD4细胞计数高的患者发展为活动性结核病的风险似乎较低。在一些患者中,尤其是基线IFN-γ水平接近临界值的患者,QFT检测结果转为阴性,与预防性抗结核治疗无关,这表明可能存在假阳性检测结果。这凸显了为免疫诊断试验定义可靠临界值以及在选定患者中推迟预防性治疗的重要性。需要进行更长随访时间的随机研究,以确定在结核病低流行地区能从LTBI治疗中获益的HIV患者。