Syddall Holly E, Westbury Leo D, Cooper Cyrus, Sayer Avan Aihie
MRC Lifecourse Epidemiology Unit, University of Southampton, Southampton General Hospital, Southampton, UK.
MRC Lifecourse Epidemiology Unit, University of Southampton, Southampton General Hospital, Southampton, UK.
J Am Med Dir Assoc. 2015 Apr;16(4):323-8. doi: 10.1016/j.jamda.2014.11.004. Epub 2014 Dec 15.
Walking speed is central to emerging consensus definitions of sarcopenia and frailty as well as being a major predictor of future health outcomes in its own right. However, measurement is not always feasible in clinical settings. We hypothesized that self-reported walking speed might be a good marker of objectively measured walking speed for use in this context.
We investigated the relationship between self-reported and measured walking speed and their associations with clinical characteristics and mortality using data from 730 men and 999 women, aged 61 to 73 years, who participated in the Hertfordshire Cohort Study. Walking speed was measured over 3 meters. Participants rated their walking speed as "unable to walk," "very slow," "stroll at an easy pace," "normal speed," "fairly brisk," or "fast."
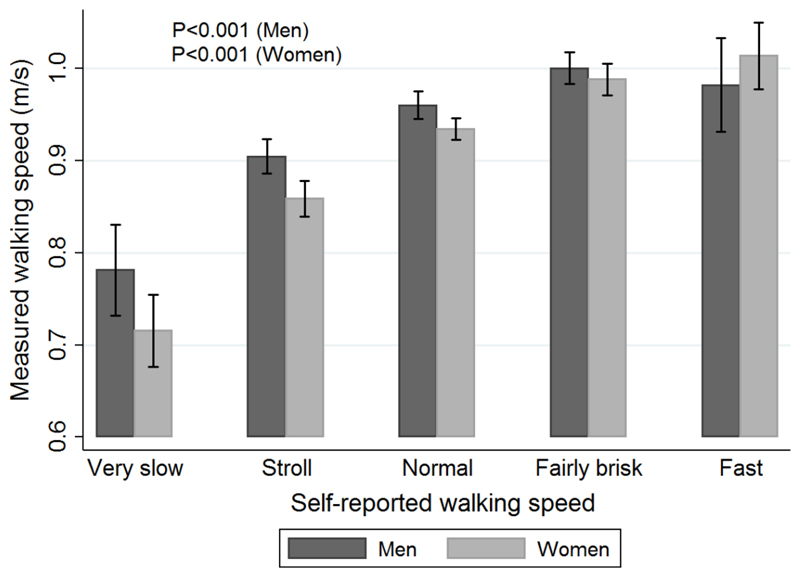
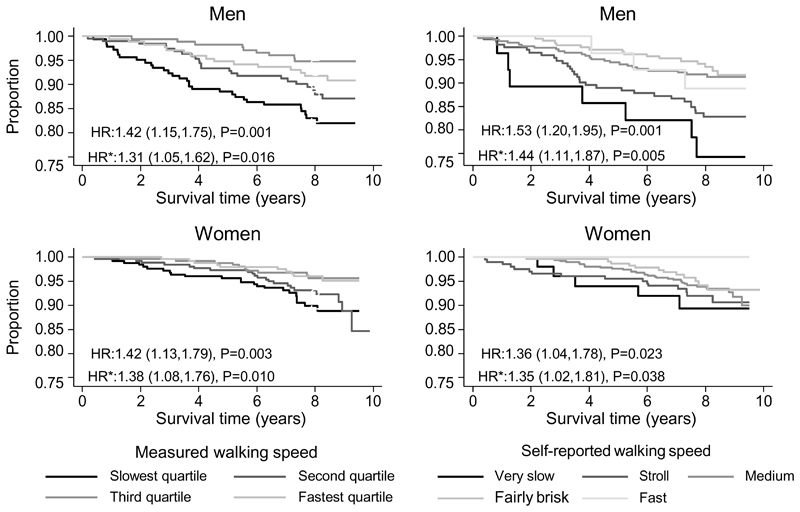
Self-reported walking speed was strongly associated with measured walking speed among men and women (P < .001). Average walking speeds ranged from 0.78 m/s (95% CI 0.73-0.83) among men with "very slow" self-reported walking speed to 0.98 m/s (95% CI 0.93-1.03) among "fast" walkers (corresponding figures for women were 0.72 m/s [95% CI 0.68-0.75] and 1.01 m/s [95% CI 0.98-1.05]). Self-reported and measured walking speeds were similarly associated with clinical characteristics and mortality; among men and women, slower self-reported and measured walking speeds were associated (P < .05) with increased likelihood of poor physical function, having more systems medicated and with increased mortality risk, with and without adjustment for sociodemographic and lifestyle factors (hazard ratios for mortality per slower band of self-reported walking speed, adjusted for sociodemographic and lifestyle characteristics: men 1.44 [95% CI 1.11-1.87]; women 1.35 [95% CI 1.02-1.81]).
Self-reported walking speed is a good marker of measured walking speed and could serve as a useful marker of physical performance in consensus definitions of sarcopenia and frailty when direct measurement of walking speed is not feasible.
步行速度是肌少症和衰弱症新出现的共识定义的核心内容,其本身也是未来健康状况的主要预测指标。然而,在临床环境中测量步行速度并不总是可行的。我们假设自我报告的步行速度可能是客观测量的步行速度的一个良好指标,可用于这一背景。
我们使用来自参与赫特福德郡队列研究的730名男性和999名女性(年龄在61至73岁之间)的数据,调查了自我报告的步行速度与测量的步行速度之间的关系,以及它们与临床特征和死亡率的关联。步行速度通过3米的距离进行测量。参与者将他们的步行速度评为“无法行走”“非常慢”“轻松漫步”“正常速度”“相当轻快”或“快”。
自我报告的步行速度与男性和女性测量的步行速度密切相关(P <.001)。平均步行速度范围从自我报告步行速度为“非常慢”的男性中的0.78米/秒(95%置信区间0.73 - 0.83)到“快”步行者中的0.98米/秒(95%置信区间0.93 - 1.03);女性的相应数字为0.72米/秒(95%置信区间0.68 - 0.75)和1.01米/秒(95%置信区间0.98 - 1.05)。自我报告的步行速度和测量的步行速度与临床特征和死亡率的关联相似;在男性和女性中,自我报告和测量步行速度较慢与身体功能差、用药系统较多以及死亡率风险增加相关(P <.05),无论是否调整社会人口统计学和生活方式因素(根据自我报告步行速度每降低一个等级调整社会人口统计学和生活方式特征后的死亡率风险比:男性1.44 [95%置信区间1.11 - 1.87];女性1.35 [95%置信区间1.02 - 1.81])。
自我报告的步行速度是测量步行速度的良好指标,当步行速度直接测量不可行时,可作为肌少症和衰弱症共识定义中身体性能的有用指标。