Raman Siva P, Reddy Sushanth, Weiss Matthew J, Manos Lindsey L, Cameron John L, Zheng Lei, Herman Joseph M, Hruban Ralph H, Fishman Elliot K, Wolfgang Christopher L
1 Department of Radiology, Johns Hopkins University School of Medicine, JHOC 3251, 601 N Caroline St, Baltimore, MD 21287.
AJR Am J Roentgenol. 2015 Jan;204(1):W37-42. doi: 10.2214/AJR.13.12439.
Pancreatic adenocarcinoma is a rapidly progressive malignancy characterized by its tendency for early metastatic spread. MDCT is the primary diagnostic modality for the preoperative staging of patients with pancreatic cancer, with an accuracy established in multiple studies. However, for a variety of reasons, there is often a prolonged interval between staging MDCT and the surgical intervention. This study examines the relationship between the interval between imaging and surgery and the accuracy of MDCT in determining the presence or absence of metastatic disease at surgery in patients with pancreatic cancer.
Patients were identified who had undergone surgery for pancreatic cancer at our institution with a dedicated preoperative pancreas-protocol MDCT performed in our department. Findings from the preoperative MDCT report were correlated with the operative findings, as well as the time between imaging and surgery.
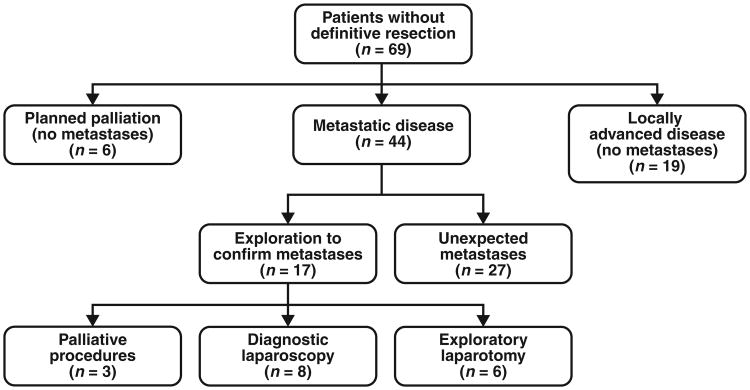
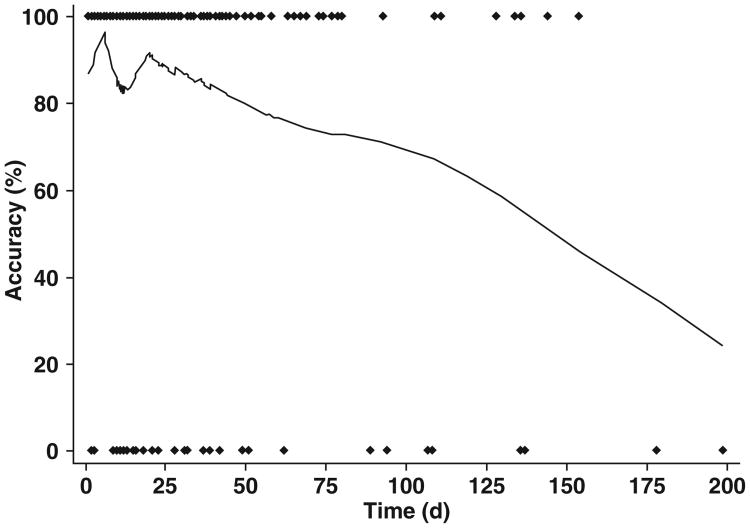
Two hundred ninety-two MDCT scans were performed on 256 patients who underwent exploration for pancreatic adenocarcinoma. The patients had a median age of 67 years (range, 30-95 years), and 51.6% (132/256) were male. The median time between MDCT and surgical exploration was 15.5 days (range, 1-198 days). MDCT correctly predicted the absence of metastatic disease at surgery in 233 of 274 (85.0%) studies. MDCT was more accurate in predicting the absence of metastatic disease if the study was performed within 25 days of surgery than it was if the study was performed within more than 25 days of surgery (89.3% vs 77.0%; p = 0.0097). Furthermore, regression models showed that the negative predictive value of a given MDCT significantly decreased after approximately 4 weeks.
MDCT is an accurate method to stage patients with pancreatic cancer, but its accuracy in excluding distant metastatic disease depreciates over time. Patients should undergo a repeat MDCT within 25 days of any planned definitive operative intervention for pancreatic cancer to avoid unexpectedly finding metastatic disease at surgery.
胰腺腺癌是一种进展迅速的恶性肿瘤,其特点是易于早期发生转移扩散。多排螺旋CT(MDCT)是胰腺癌患者术前分期的主要诊断方法,多项研究已证实其准确性。然而,由于各种原因,分期MDCT与手术干预之间往往存在较长间隔。本研究探讨了影像检查与手术之间的间隔时间与MDCT在确定胰腺癌患者手术时是否存在转移疾病的准确性之间的关系。
确定在我院接受胰腺癌手术且在我科进行了专门的术前胰腺方案MDCT检查的患者。术前MDCT报告的结果与手术结果以及影像检查与手术之间的时间进行了对比。
对256例接受胰腺腺癌探查的患者进行了292次MDCT扫描。患者的中位年龄为67岁(范围30 - 95岁),51.6%(132/256)为男性。MDCT与手术探查之间的中位时间为15.5天(范围1 - 198天)。在274项研究中的233项(85.0%)中,MDCT正确预测了手术时无转移疾病。如果在手术25天内进行MDCT检查,其预测无转移疾病的准确性高于在手术25天以上进行检查时(89.3%对77.0%;p = 0.0097)。此外,回归模型显示,大约4周后,给定MDCT的阴性预测值显著下降。
MDCT是对胰腺癌患者进行分期的准确方法,但其排除远处转移疾病的准确性会随着时间降低。对于任何计划进行的胰腺癌确定性手术干预,患者应在25天内接受重复MDCT检查,以避免手术时意外发现转移疾病。