Njuguna Henry N, Caselton Deborah L, Arunga Geoffrey O, Emukule Gideon O, Kinyanjui Dennis K, Kalani Rosalia M, Kinkade Carl, Muthoka Phillip M, Katz Mark A, Mott Joshua A
Influenza Program, Centers for Disease Control and Prevention-Kenya, P.O. Box 606, 00621, Village Market, Nairobi, Kenya.
Kenya Medical Research Institute (KEMRI), Nairobi, Kenya.
BMC Med Inform Decis Mak. 2014 Dec 24;14:107. doi: 10.1186/s12911-014-0107-5.
For disease surveillance, manual data collection using paper-based questionnaires can be time consuming and prone to errors. We introduced smartphone data collection to replace paper-based data collection for an influenza sentinel surveillance system in four hospitals in Kenya. We compared the quality, cost and timeliness of data collection between the smartphone data collection system and the paper-based system.
Since 2006, the Kenya Ministry of Health (MoH) with technical support from the Kenya Medical Research Institute/Centers for Disease Control and Prevention (KEMRI/CDC) conducted hospital-based sentinel surveillance for influenza in Kenya. In May 2011, the MOH replaced paper-based collection with an electronic data collection system using Field Adapted Survey Toolkit (FAST) on HTC Touch Pro2 smartphones at four sentinel sites. We compared 880 paper-based questionnaires dated Jan 2010-Jun 2011 and 880 smartphone questionnaires dated May 2011-Jun 2012 from the four surveillance sites. For each site, we compared the quality, cost and timeliness of each data collection system.
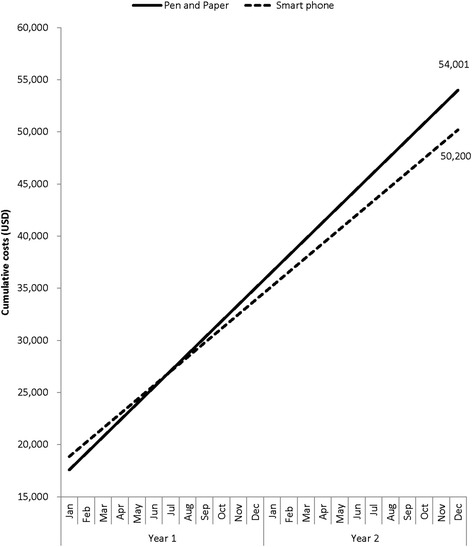
Incomplete records were more likely seen in data collected using pen-and-paper compared to data collected using smartphones (adjusted incidence rate ratio (aIRR) 7, 95% CI: 4.4-10.3). Errors and inconsistent answers were also more likely to be seen in data collected using pen-and-paper compared to data collected using smartphones (aIRR: 25, 95% CI: 12.5-51.8). Smartphone data was uploaded into the database in a median time of 7 days while paper-based data took a median of 21 days to be entered (p < 0.01). It cost USD 1,501 (9.4%) more to establish the smartphone data collection system ($17,500) than the pen-and-paper system (USD $15,999). During two years, however, the smartphone data collection system was $3,801 (7%) less expensive to operate ($50,200) when compared to pen-and-paper system ($54,001).
Compared to paper-based data collection, an electronic data collection system produced fewer incomplete data, fewer errors and inconsistent responses and delivered data faster. Although start-up costs were higher, the overall costs of establishing and running the electronic data collection system were lower compared to paper-based data collection system. Electronic data collection using smartphones has potential to improve timeliness, data integrity and reduce costs.
在疾病监测中,使用纸质问卷进行人工数据收集可能既耗时又容易出错。我们引入了智能手机数据收集方式,以取代肯尼亚四家医院流感哨点监测系统中的纸质数据收集。我们比较了智能手机数据收集系统和纸质系统在数据收集的质量、成本和及时性方面的差异。
自2006年以来,肯尼亚卫生部在肯尼亚医学研究所/疾病控制与预防中心(KEMRI/CDC)的技术支持下,在肯尼亚开展了基于医院的流感哨点监测。2011年5月,卫生部在四个哨点用HTC Touch Pro2智能手机上使用现场适应性调查工具包(FAST)的电子数据收集系统取代了纸质收集。我们比较了2010年1月至2011年6月的880份纸质问卷和2011年5月至2012年6月来自四个监测点的880份智能手机问卷。对于每个站点,我们比较了每个数据收集系统的质量、成本和及时性。
与使用智能手机收集的数据相比,使用纸笔收集的数据中不完整记录更为常见(调整发病率比(aIRR)为7,95%置信区间:4.4-10.3)。与使用智能手机收集的数据相比,使用纸笔收集的数据中错误和不一致答案也更常见(aIRR:25,95%置信区间:12.5-51.8)。智能手机数据上传到数据库的中位时间为7天,而纸质数据录入的中位时间为21天(p<0.01)。建立智能手机数据收集系统(17500美元)比纸笔系统(15999美元)多花费1501美元(9.4%)。然而,在两年时间里,与纸笔系统(54001美元)相比,智能手机数据收集系统的运营成本低3801美元(7%)(50200美元)。
与纸质数据收集相比,电子数据收集系统产生的不完整数据更少、错误和不一致回答更少,且数据交付更快。虽然启动成本较高,但与纸质数据收集系统相比,建立和运行电子数据收集系统的总体成本更低。使用智能手机进行电子数据收集有潜力提高及时性、数据完整性并降低成本。