Min Jin Hye, Lee Sang Eun, Lee Hong Sik, Chae Young Keun, Lee Yong Kyung, Kang Yoo, Je Ui Jin
Department of Anesthesiology and Pain Medicine, Myongji Hospital, Goyang, Korea.
Korean J Anesthesiol. 2014 Dec;67(6):378-83. doi: 10.4097/kjae.2014.67.6.378. Epub 2014 Dec 29.
The stroke volume variation (SVV), based on lung-heart interaction during mechanical ventilation, is a useful dynamic parameter for fluid responsiveness. However, it is affected by many factors. The aim of this study was to evaluate the effects of SVV on Trendelenburg (T) and reverse Trendelenburg (RT) position and to further elaborate on the patterns of the SVV with position.
Forty-two patients undergoing elective surgery were enrolled in this study. Fifteen minutes after standardized induction of anesthesia with propofol, fentanyl, and rocuronium with volume controlled ventilation (tidal volume of 8 ml/kg of ideal body weight, inspiration : expiration ratio of 1 : 2, and respiratory rate of 10-13 breaths/min), the patients underwent posture changes as follows: supine, T position at slopes of operating table of -5°, -10°, and -15°, and RT position at slopes of operating table of 5°, 10°, and 15°. At each point, SVV, cardiac output (CO), peak airway pressure (PAP), mean blood pressure, and heart rate (HR) were recorded.
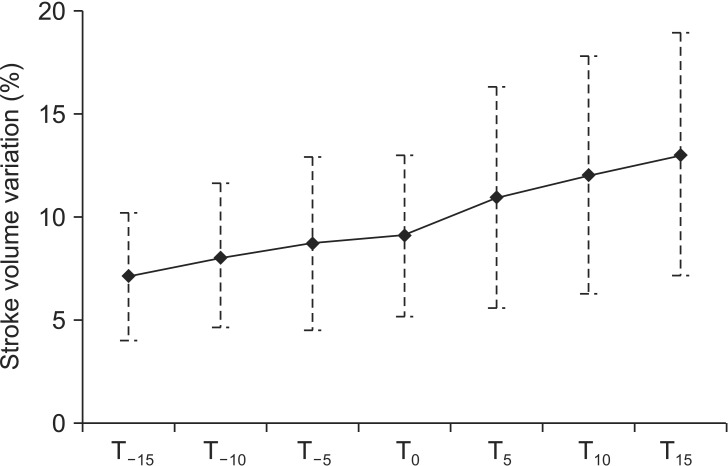
The SVV was significant decreased with decreased slopes of operating table in T position, and increased with increased slopes of operating table in RT position (P = 0.000). Schematically, it was increased by 1% when the slope of operating table was increased by 5°. But, the CO and PAP were significant increased with decreased slopes of operating table in T position, and decreased with increased slopes of operating table in RT position (P = 0.045, 0.027).
SVV is subjected to the posture, and we should take these findings into account on reading SVV for fluid therapy.
基于机械通气期间肺心相互作用的每搏输出量变异(SVV)是用于评估液体反应性的一个有用的动态参数。然而,它受多种因素影响。本研究的目的是评估SVV在头低脚高位(T)和头高脚低位(RT)时的变化,并进一步阐述SVV随体位变化的模式。
42例择期手术患者纳入本研究。在使用丙泊酚、芬太尼和罗库溴铵进行标准化麻醉诱导并采用容量控制通气(潮气量为理想体重的8 ml/kg,吸呼比为1∶2,呼吸频率为10~13次/分钟)15分钟后,患者进行如下体位改变:仰卧位、手术台倾斜角度为-5°、-10°和-15°的头低脚高位,以及手术台倾斜角度为5°、10°和15°的头高脚低位。在每个体位点,记录SVV、心输出量(CO)、气道峰压(PAP)、平均血压和心率(HR)。
在头低脚高位时,随着手术台倾斜角度减小,SVV显著降低;在头高脚低位时,随着手术台倾斜角度增加,SVV升高(P = 0.000)。具体而言,手术台倾斜角度每增加5°,SVV增加1%。但是,在头低脚高位时,随着手术台倾斜角度减小,CO和PAP显著升高;在头高脚低位时,随着手术台倾斜角度增加,CO和PAP降低(P = 0.045,0.027)。
SVV受体位影响,我们在解读用于液体治疗的SVV时应考虑这些发现。