Westbrook Johanna I, Li Ling, Lehnbom Elin C, Baysari Melissa T, Braithwaite Jeffrey, Burke Rosemary, Conn Chris, Day Richard O
Centre for Health Systems and Safety Research, Australian Institute of Health Innovation, Faculty of Medicine and Health Sciences, Macquarie University, Sydney 2109, Australia.
Centre for Healthcare Resilience and Implementation Science, Australian Institute of Health Innovation, Faculty of Medicine and Health Sciences, Macquarie University, Sydney 2109, Australia.
Int J Qual Health Care. 2015 Feb;27(1):1-9. doi: 10.1093/intqhc/mzu098. Epub 2015 Jan 12.
To (i) compare medication errors identified at audit and observation with medication incident reports; (ii) identify differences between two hospitals in incident report frequency and medication error rates; (iii) identify prescribing error detection rates by staff.
Audit of 3291 patient records at two hospitals to identify prescribing errors and evidence of their detection by staff. Medication administration errors were identified from a direct observational study of 180 nurses administering 7451 medications. Severity of errors was classified. Those likely to lead to patient harm were categorized as 'clinically important'.
Two major academic teaching hospitals in Sydney, Australia.
Rates of medication errors identified from audit and from direct observation were compared with reported medication incident reports.
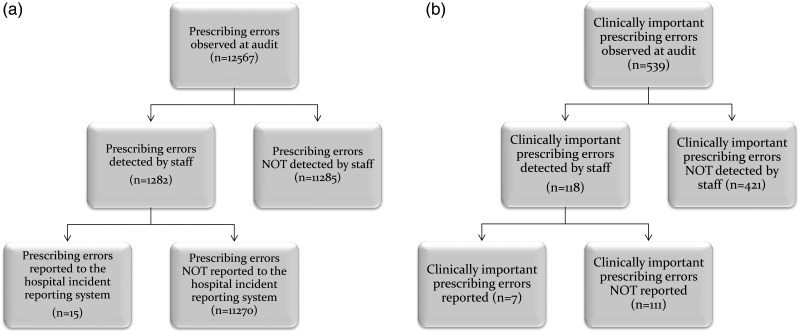
A total of 12 567 prescribing errors were identified at audit. Of these 1.2/1000 errors (95% CI: 0.6-1.8) had incident reports. Clinically important prescribing errors (n = 539) were detected by staff at a rate of 218.9/1000 (95% CI: 184.0-253.8), but only 13.0/1000 (95% CI: 3.4-22.5) were reported. 78.1% (n = 421) of clinically important prescribing errors were not detected. A total of 2043 drug administrations (27.4%; 95% CI: 26.4-28.4%) contained ≥ 1 errors; none had an incident report. Hospital A had a higher frequency of incident reports than Hospital B, but a lower rate of errors at audit.
Prescribing errors with the potential to cause harm frequently go undetected. Reported incidents do not reflect the profile of medication errors which occur in hospitals or the underlying rates. This demonstrates the inaccuracy of using incident frequency to compare patient risk or quality performance within or across hospitals. New approaches including data mining of electronic clinical information systems are required to support more effective medication error detection and mitigation.
(i)比较审核和观察中发现的用药错误与用药事件报告;(ii)确定两家医院在事件报告频率和用药错误率方面的差异;(iii)确定工作人员的处方错误检测率。
对两家医院的3291份患者记录进行审核,以确定处方错误及其被工作人员检测到的证据。通过对180名护士给药7451次的直接观察研究确定用药错误。对错误的严重程度进行分类。那些可能导致患者伤害的被归类为“具有临床重要性”。
澳大利亚悉尼的两家主要学术教学医院。
将审核和直接观察中发现的用药错误率与报告的用药事件报告进行比较。
审核中总共发现12567处处方错误。其中,每1000处错误中有1.2处(95%可信区间:0.6 - 1.8)有事件报告。具有临床重要性的处方错误(n = 539)被工作人员检测到的比例为每1000处中有218.9处(95%可信区间:184.0 - 253.8),但只有每1000处中的13.0处(95%可信区间:3.4 - 22.5)有报告。78.1%(n = 421)具有临床重要性的处方错误未被检测到。总共2043次给药(27.4%;95%可信区间:26.4 - 28.4%)包含≥1处错误;均无事件报告。医院A的事件报告频率高于医院B,但审核中的错误率较低。
有可能造成伤害的处方错误经常未被发现。报告的事件并不能反映医院中发生的用药错误情况或潜在发生率。这表明使用事件频率来比较医院内部或不同医院之间的患者风险或质量表现是不准确的。需要新的方法,包括对电子临床信息系统进行数据挖掘,以支持更有效的用药错误检测和缓解。