Van Craenenbroeck Amaryllis H, Van Ackeren Katrijn, Hoymans Vicky Y, Roeykens Johan, Verpooten Gert A, Vrints Christiaan J, Couttenye Marie M, Van Craenenbroeck Emeline M
Laboratory of Cellular and Molecular Cardiology, Antwerp University Hospital, 2650 Antwerp, Belgium ; Department of Nephrology, Antwerp University Hospital, 2650 Antwerp, Belgium ; Laboratory of Experimental Medicine and Pediatrics, University of Antwerp, 2650 Antwerp, Belgium.
Cardiovascular Diseases, Department of Translational Pathophysiological Research, University of Antwerp, 2650 Antwerp, Belgium.
Mediators Inflamm. 2014;2014:216534. doi: 10.1155/2014/216534. Epub 2014 Dec 22.
Monocytes (Mon1-2-3) play a substantial role in low-grade inflammation associated with high cardiovascular morbidity and mortality of patients with chronic kidney disease (CKD) and chronic heart failure (CHF). The effect of an acute exercise bout on monocyte subsets in the setting of systemic inflammation is currently unknown. This study aims (1) to evaluate baseline distribution of monocyte subsets in CHF and CKD versus healthy subjects (HS) and (2) to evaluate the effect of an acute exercise bout. Exercise-induced IL-6 and MCP-1 release are related to the Mon1-2-3 response.
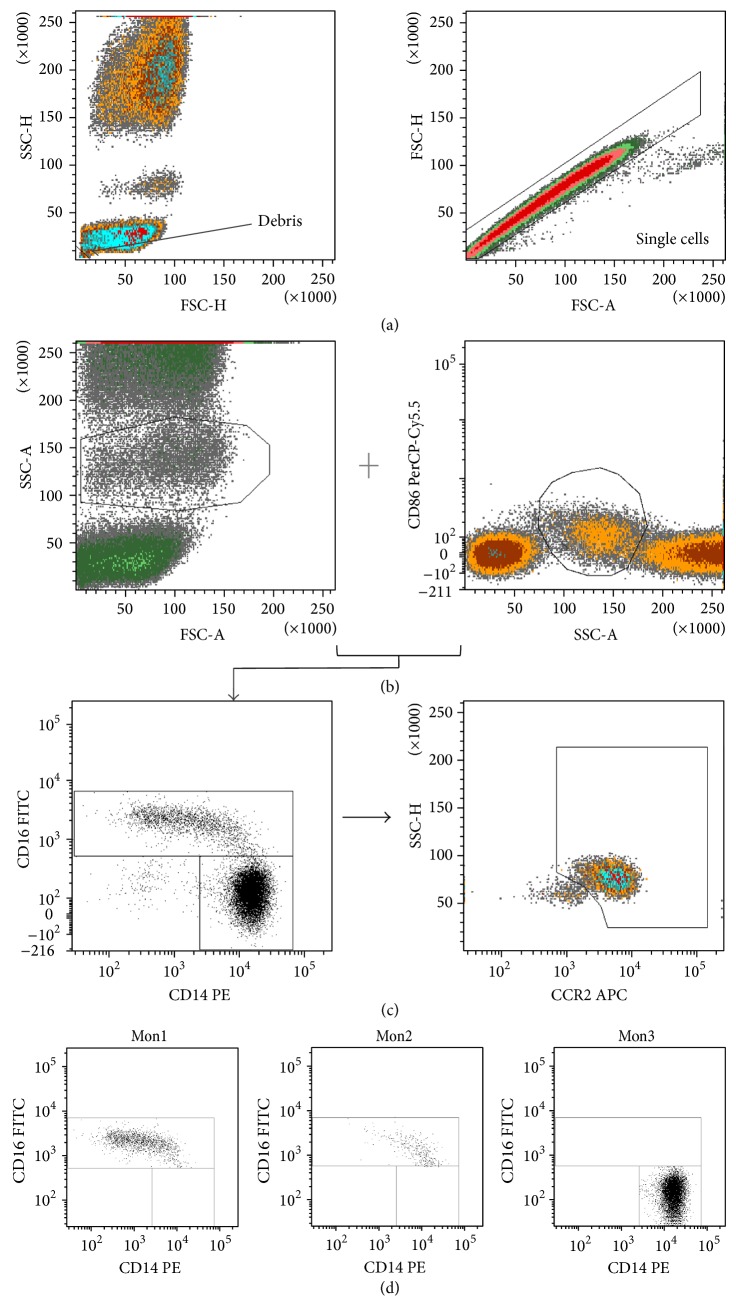
Twenty CHF patients, 20 CKD patients, and 15 HS were included. Before and after a maximal cardiopulmonary exercise test, monocyte subsets were quantified by flow cytometry: CD14(++)CD16(-)CCR2(+) (Mon1), CD14(++)CD16(+)CCR2(+) (Mon2), and CD14(+)CD16(++)CCR2(-) (Mon3). Serum levels of IL-6 and MCP-1 were determined by ELISA.
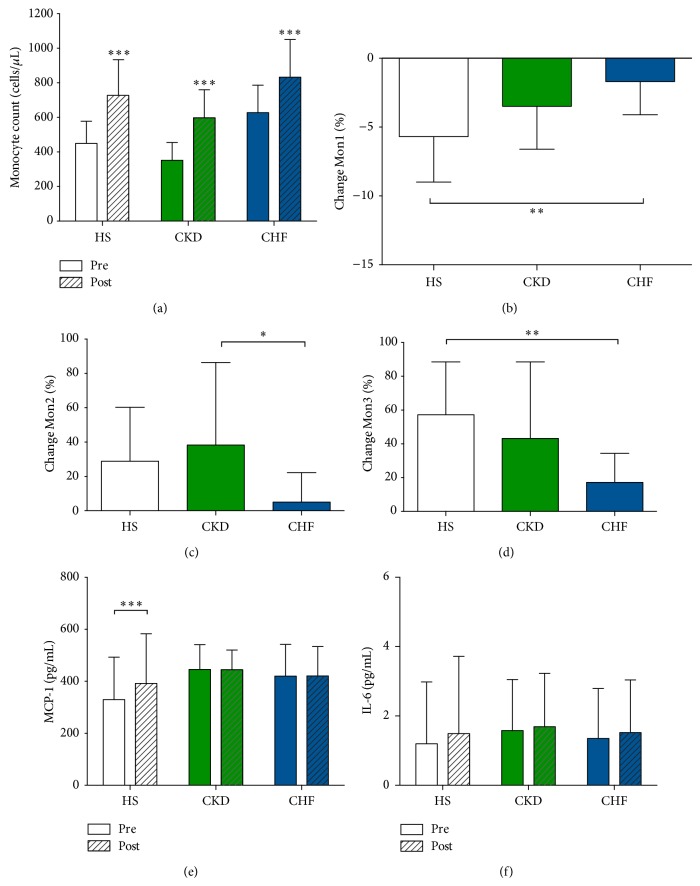
Baseline distribution of Mon1-2-3 was comparable between the 3 groups. Following acute exercise, %Mon2 and %Mon3 increased significantly at the expense of a decrease in %Mon1 in HS and in CKD. This response was significantly attenuated in CHF (P < 0.05). In HS only, MCP-1 levels increased following exercise; IL-6 levels were unchanged. Circulatory power was a strong and independent predictor of the changes in Mon1 (β = -0.461, P < 0.001) and Mon3 (β = 0.449, P < 0.001); and baseline LVEF of the change in Mon2 (β = 0.441, P < 0.001).
The response of monocytes to acute exercise is characterized by an increase in proangiogenic and proinflammatory Mon2 and Mon3 at the expense of phagocytic Mon1. This exercise-induced monocyte subset response is mainly driven by hemodynamic changes and not by preexistent low-grade inflammation.
单核细胞(Mon1 - 2 - 3)在与慢性肾脏病(CKD)和慢性心力衰竭(CHF)患者高心血管发病率及死亡率相关的低度炎症中起重要作用。目前尚不清楚急性运动对全身炎症背景下单核细胞亚群的影响。本研究旨在(1)评估CHF和CKD患者与健康受试者(HS)之间单核细胞亚群的基线分布,以及(2)评估急性运动的影响。运动诱导的白细胞介素 - 6(IL - 6)和单核细胞趋化蛋白 - 1(MCP - 1)释放与Mon1 - 2 - 3反应相关。
纳入20例CHF患者、20例CKD患者和15例HS。在最大心肺运动试验前后,通过流式细胞术对单核细胞亚群进行定量:CD14(++)CD16(-)CCR2(+)(Mon1)、CD14(++)CD16(+)CCR2(+)(Mon2)和CD14(+)CD16(++)CCR2(-)(Mon3)。通过酶联免疫吸附测定法(ELISA)测定血清IL - 6和MCP - 1水平。
三组之间Mon1 - 2 - 3的基线分布相当。急性运动后,HS和CKD患者中,%Mon2和%Mon3显著增加而%Mon1减少。CHF患者中这种反应明显减弱(P < 0.05)。仅在HS中,运动后MCP - 1水平升高;IL - 6水平未改变。循环功率是Mon1变化(β = -0.461,P < 0.001)和Mon3变化(β = 0.449,P < 0.001)的强且独立的预测因子;基线左心室射血分数(LVEF)是Mon2变化的预测因子(β = 0.441,P < 0.001)。
单核细胞对急性运动的反应特征是促血管生成和促炎的Mon2和Mon3增加,以吞噬性的Mon1减少为代价。这种运动诱导的单核细胞亚群反应主要由血流动力学变化驱动,而非由先前存在的低度炎症驱动。