Moinuddin Zia, Summers Angela, Van Dellen David, Augustine Titus, Herrick Sarah E
Department of Transplantation, Manchester Royal Infirmary Manchester, UK ; Faculty of Medical and Human Sciences, Institute of Inflammation and Repair, University of Manchester, Manchester Academic Health Science Centre Manchester, UK.
Department of Transplantation, Manchester Royal Infirmary Manchester, UK.
Front Physiol. 2015 Jan 5;5:470. doi: 10.3389/fphys.2014.00470. eCollection 2014.
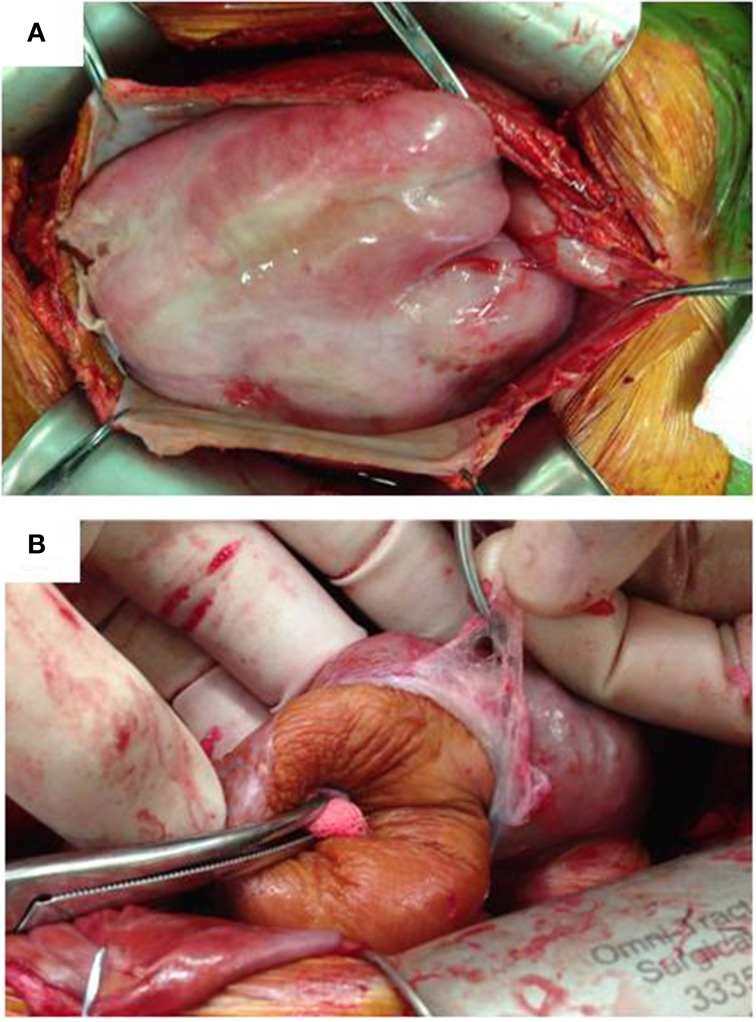
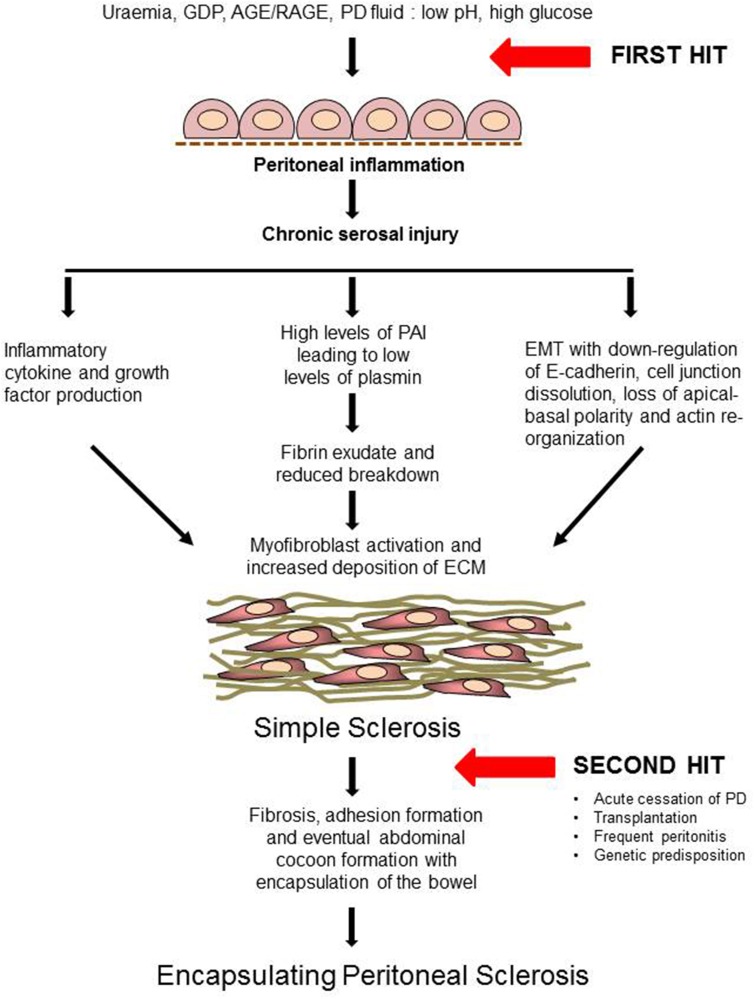
Encapsulating peritoneal sclerosis (EPS) is a devastating but, fortunately, rare complication of long-term peritoneal dialysis. The disease is associated with extensive thickening and fibrosis of the peritoneum resulting in the formation of a fibrous cocoon encapsulating the bowel leading to intestinal obstruction. The incidence of EPS ranges between 0.7 and 3.3% and increases with duration of peritoneal dialysis therapy. Dialysis fluid is hyperosmotic, hyperglycemic, and acidic causing chronic injury and inflammation in the peritoneum with loss of mesothelium and extensive tissue fibrosis. The pathogenesis of EPS, however, still remains uncertain, although a widely accepted hypothesis is the "two-hit theory," where, the first hit is chronic peritoneal membrane injury from long standing peritoneal dialysis followed by a second hit such as an episode of peritonitis, genetic predisposition and/or acute cessation of peritoneal dialysis, leading to EPS. Recently, EPS has been reported in patients shortly after transplantation suggesting that this procedure may also act as a possible second insult. The process of epithelial-mesenchymal transition of mesothelial cells is proposed to play a central role in the development of peritoneal sclerosis, a common characteristic of patients on dialysis, however, its importance in EPS is less clear. There is no established treatment for EPS although evidence from small case studies suggests that corticosteroids and tamoxifen may be beneficial. Nutritional support is essential and surgical intervention (peritonectomy and enterolysis) is recommended in later stages to relieve bowel obstruction.
包裹性腹膜硬化症(EPS)是长期腹膜透析中一种严重但幸运的是较为罕见的并发症。该疾病与腹膜广泛增厚和纤维化相关,导致形成包裹肠道的纤维性茧,进而引起肠梗阻。EPS的发病率在0.7%至3.3%之间,并随着腹膜透析治疗时间的延长而增加。透析液具有高渗性、高血糖性和酸性,会导致腹膜慢性损伤和炎症,伴有间皮细胞丢失和广泛的组织纤维化。然而,尽管广泛接受的假说是“二次打击理论”,即第一次打击是长期腹膜透析导致的慢性腹膜损伤,随后第二次打击如腹膜炎发作、遗传易感性和/或腹膜透析突然停止,从而导致EPS,但EPS的发病机制仍不确定。最近,有报道称移植后不久的患者也出现了EPS,这表明该手术也可能是一种潜在的二次损伤。间皮细胞的上皮-间质转化过程被认为在腹膜硬化的发展中起核心作用,腹膜硬化是透析患者的一个共同特征,然而其在EPS中的重要性尚不清楚。目前尚无针对EPS的确立治疗方法,尽管小病例研究的证据表明皮质类固醇和他莫昔芬可能有益。营养支持至关重要,后期建议进行手术干预(腹膜切除术和肠粘连松解术)以缓解肠梗阻。