Craven E Randy
Glaucma Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia.
Middle East Afr J Ophthalmol. 2015 Jan-Mar;22(1):30-7. doi: 10.4103/0974-9233.148346.
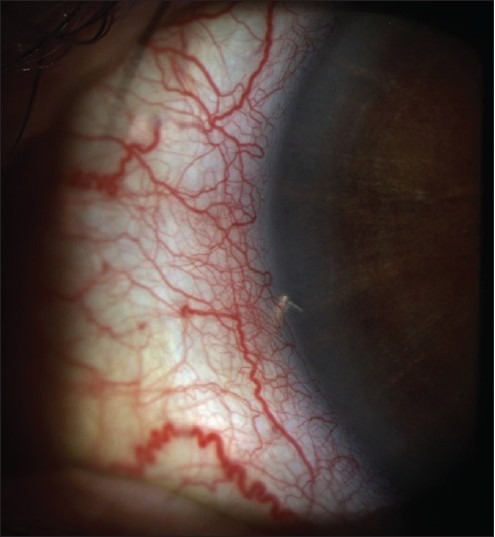
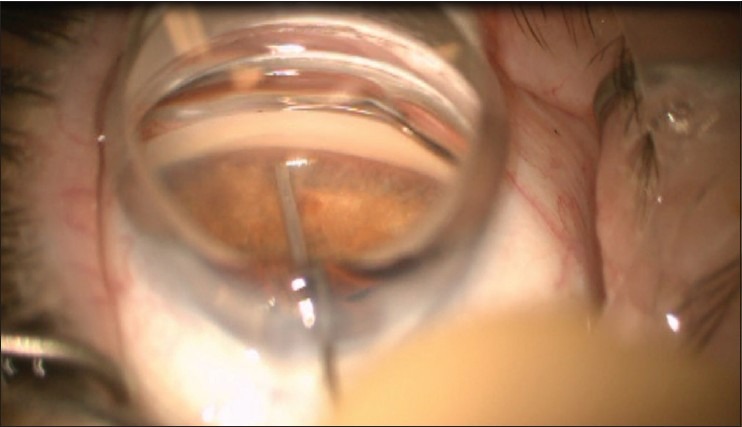
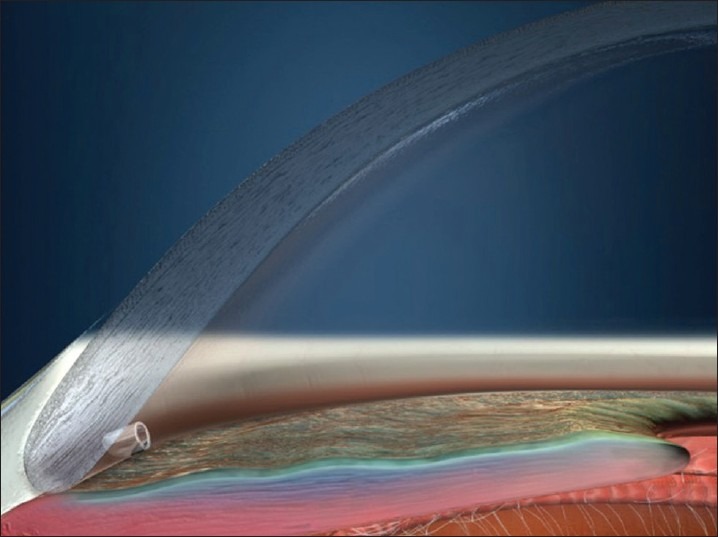
The trabecular bypass stent offers an alternative to filtration surgery. Patients who may be ideal candidates for considering this procedure are those with prior conjunctival surgery; for example, those who had a 360° peritomy from a scleral buckle might not do well with a trabeculectomy and there is no space for a tube. Highly myopic patients do not tolerate hypotony well, and the iSTB may be an option for some of these patients. I have used the iSTB in patients on anticoagulants who could not stop them, and they needed something beyond medications and laser to lower the IOP in subjects with open-angle glaucoma. Young patients, especially those with one eye, who need rapid visual recovery (for instance to return to work) may be good candidates to consider the iSTB as well. Because of the position used for clear corneal cataract surgery, the temporal approach is best for doing these. Therefore, if you are doing cataract surgery on someone who needs a lower IOP, you already are in the correct position to implant the devices. Patients may need some medications after the procedure to lower the IOP to the level desired. The results from Armenia are encouraging, given an IOP of 11.8 mmHg after 2 iSTB stents and taking daily travoprost. These results are difficult to reach even with a trabeculectomy. When selecting your fist patients, avoid those with the congested episcleral veins, look for patients with wide open angles, and if you can see aqueous veins at the slit-lamp it may indicate a viable outflow system. Probably avoid patients with IOPs over 35 mmHg. The micro-invasive trabecular bypass stents offer an alternative surgical intervention for select patients with open-angle glaucoma. Recent studies show that combining these micro-stents with medications can lead to as low of an intraocular pressure (IOP) as is achieved by many more invasive incisional surgeries. The technique is quite precise and learning the procedure is similar to clear corneal phacoemulsification followed by a goniotomy. Long-term data are starting to come in and the safety is favorable. The IOP success appears to be based on the patency of the outflow system for a given patient. Key factors in determining the success involve the placement of trabecular bypass devices into the canal of Schlemm and require a down-stream patency of the collector channel system and a low episcleral venous pressure. Because accessing the collector system may require placement by a patent channel, the placement of two stents, a longer stent with scaffolding or somehow imaging the outflow system may lead to the best control of the IOP.
小梁旁路支架为滤过性手术提供了一种替代方案。可能适合考虑该手术的理想患者是那些曾接受过结膜手术的人;例如,那些因巩膜扣带术而进行了360°球结膜环切术的患者,小梁切除术可能效果不佳,且没有放置引流管的空间。高度近视患者对低眼压耐受性较差,iSTB(一种小梁旁路支架)可能是其中一些患者的选择。我曾在无法停用抗凝剂的青光眼患者中使用iSTB,对于这些开角型青光眼患者,他们需要药物和激光之外的方法来降低眼压。年轻患者,尤其是单眼患者,若需要快速恢复视力(比如重返工作岗位),也可能是考虑iSTB的合适人选。由于在透明角膜白内障手术中所采用的位置,颞侧入路最适合进行此类手术。因此,如果你正在为需要降低眼压的患者进行白内障手术,那么你已经处于植入该装置的正确位置。术后患者可能需要一些药物来将眼压降至理想水平。亚美尼亚的研究结果令人鼓舞,在植入2个iSTB支架并每日使用曲伏前列素后,眼压为11.8 mmHg。即使是小梁切除术也很难达到这样的结果。在选择首批患者时,避免选择巩膜表层静脉充血的患者,寻找房角开放宽的患者,如果你在裂隙灯下能看到房水静脉,这可能表明存在可行的房水流出系统。可能也要避免眼压超过35 mmHg的患者。微创小梁旁路支架为特定的开角型青光眼患者提供了一种替代性的手术干预方法。最近的研究表明,将这些微型支架与药物联合使用可使眼压降低到与许多更具侵入性的切开手术相当的水平。该技术非常精确,学习该手术类似于透明角膜超声乳化术加房角切开术。长期数据开始出现,安全性良好。眼压控制成功似乎取决于特定患者房水流出系统的通畅性。决定成功的关键因素包括将小梁旁路装置放置到施莱姆管中,并且需要集合管系统下游通畅以及巩膜表层静脉压较低。由于进入集合管系统可能需要通过一个开放通道进行放置,放置两个支架、一个带有支架的较长支架或者以某种方式对流出系统进行成像,可能会实现对眼压的最佳控制。