Mansbach Jonathan M, Clark Sunday, Piedra Pedro A, Macias Charles G, Schroeder Alan R, Pate Brian M, Sullivan Ashley F, Espinola Janice A, Camargo Carlos A
Department of Medicine, Boston Children's Hospital, Harvard Medical School, Boston, Massachusetts.
J Hosp Med. 2015 Apr;10(4):205-11. doi: 10.1002/jhm.2318. Epub 2015 Jan 28.
For children hospitalized with bronchiolitis, there is uncertainty about the expected inpatient clinical course and when children are safe for discharge.
Examine the time to clinical improvement, risk of clinical worsening after improvement, and develop discharge criteria.
Prospective multiyear cohort study.
Sixteen US hospitals.
Consecutive hospitalized children age <2 years with bronchiolitis.
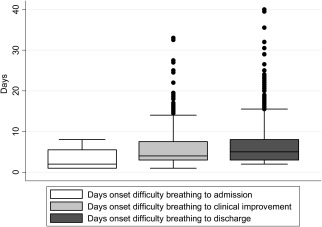
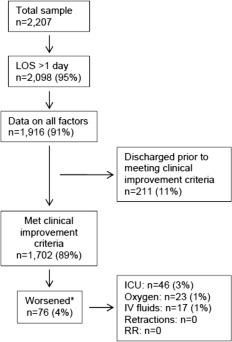
We defined clinical improvement using: (1) retraction severity, (2) respiratory rate, (3) room air oxygen saturation, and (4) hydration status. After meeting improvement criteria, children were considered clinically worse based on the inverse of ≥1 of these criteria or need for intensive care.
Among 1916 children, the median number of days from onset of difficulty breathing until clinical improvement was 4 (interquartile range, 3-7.5 days). Of the total, 1702 (88%) met clinical improvement criteria, with 4% worsening (3% required intensive care). Children who worsened were age <2 months (adjusted odds ratio [AOR]: 3.51; 95% confidence interval [CI]: 2.07-5.94), gestational age <37 weeks (AOR: 1.94; 95% CI: 1.13-3.32), and presented with severe retractions (AOR: 5.55; 95% CI: 2.12-14.50), inadequate oral intake (AOR: 2.54; 95% CI: 1.39-4.62), or apnea (AOR: 2.87; 95% CI: 1.45-5.68). Readmissions were similar for children who did and did not worsen.
Although children hospitalized with bronchiolitis had wide-ranging recovery times, only 4% worsened after initial improvement. Children who worsened were more likely to be younger, premature infants presenting in more severe distress. For children hospitalized with bronchiolitis, these data may help establish more evidence-based discharge criteria, reduce practice variability, and safely shorten hospital length-of-stay.
对于因细支气管炎住院的儿童,预期的住院临床病程以及何时出院安全尚不确定。
研究临床改善时间、改善后临床恶化风险,并制定出院标准。
前瞻性多年队列研究。
美国16家医院。
年龄小于2岁、因细支气管炎连续住院的儿童。
我们使用以下指标定义临床改善:(1)凹陷严重程度,(2)呼吸频率,(3)室内空气氧饱和度,(4)水合状态。达到改善标准后,若这些标准中至少有一项指标情况变差或需要重症监护,则儿童被视为临床恶化。
在1916名儿童中,从呼吸困难发作到临床改善的天数中位数为4天(四分位间距为3 - 7.5天)。其中,1702名(88%)达到临床改善标准,4%出现恶化(3%需要重症监护)。恶化的儿童年龄小于2个月(调整优势比[AOR]:3.51;95%置信区间[CI]:2.07 - 5.94)、胎龄小于37周(AOR:1.94;95% CI:1.13 - 3.32),且有严重凹陷(AOR:5.55;95% CI:2.12 - 14.50)、经口摄入量不足(AOR:2.54;95% CI:1.39 - 4.62)或呼吸暂停(AOR:2.87;95% CI:1.45 - 5.68)。恶化和未恶化的儿童再入院情况相似。
尽管因细支气管炎住院儿童的恢复时间差异很大,但仅4%在初始改善后出现恶化。恶化的儿童更可能是年龄较小的早产儿,病情更严重。对于因细支气管炎住院的儿童,这些数据可能有助于建立更多基于证据的出院标准,减少实践差异,并安全缩短住院时间。