Vejakama Phisitt, Ingsathit Atiporn, Attia John, Thakkinstian Ammarin
From the Section for Clinical Epidemiology and Biostatistics, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok (PV, AI, AT); Department of Medicine, Bundarik Hospital, Bundarik District, Ubon Ratchathani Province, Thailand (PV); and Centre for Clinical Epidemiology and Biostatistics, School of Medicine and Public Health, University of Newcastle, and Hunter Medical Research Institute, Newcastle, NSW, Australia (JA).
Medicine (Baltimore). 2015 Jan;94(4):e475. doi: 10.1097/MD.0000000000000475.
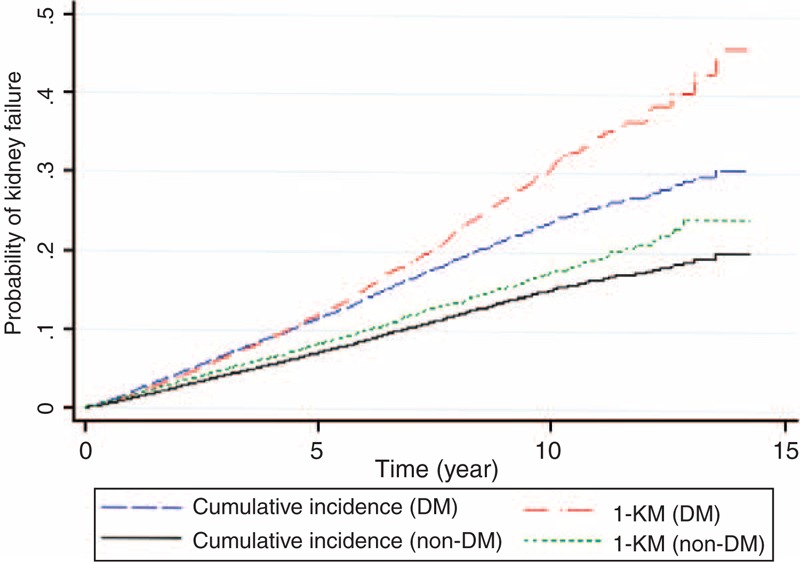
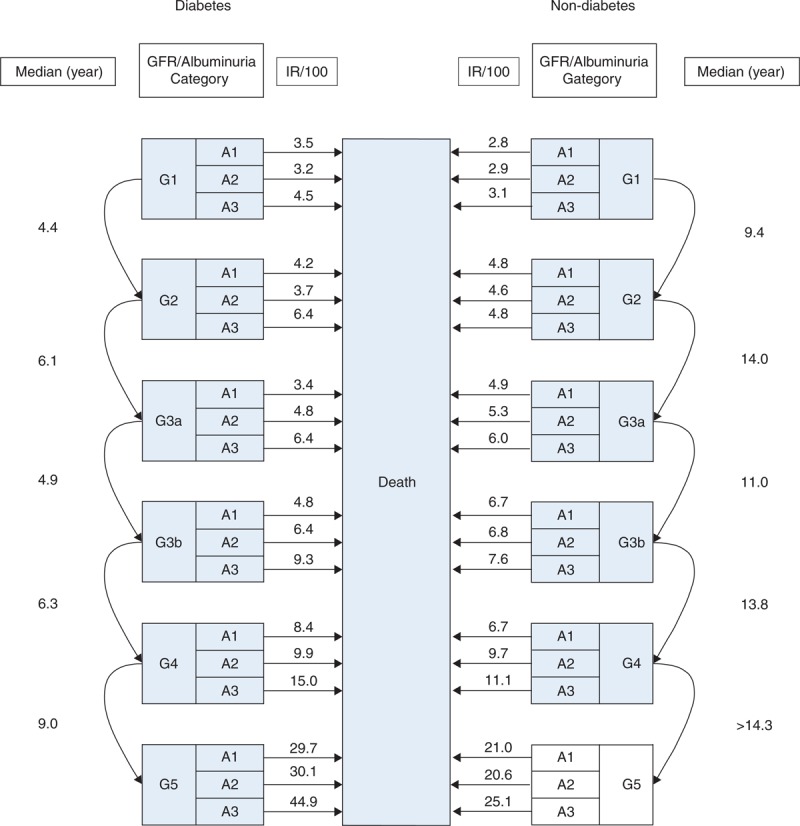
The prognostic information about CKD progression, particularly for GFR categories 1 and 2, is still limited. This cohort was therefore conducted to determine the CKD progression using a competing risk approach. We conducted a retrospective cohort study linking community health screening with hospitals and death registry data in a province of Thailand, from 1997 to 2011. A competing risk model was applied by treating death as a competing risk factor to estimate 2-, 5-, and 10-year probability of kidney failure and median time for CKD progression from lower to higher GFR category. There were 17,074 non-diabetic and 15,032 diabetic CKD subjects. Diabetic subjects progressed more rapidly through GFR categories with the median times for CKD progression from GFR categories G1 to G2, G2 to G3a, G3a to G3b, G3b to G4, and G4 to G5 of 4.4, 6.1, 4.9, 6.3, and 9.0 years, respectively. Non-diabetic subjects took longer to progress with the corresponding median time of 9.4, 14.0, 11.0, 13.8, and >14.3 years. After adjusting for confounders, diabetic subjects were 49% (cause-specific hazard ratio ((c)HR) = 1.49, 95% CI: 1.37, 1.62) more likely to develop kidney failure than non-diabetic subjects. Albuminuria categories A3 and A2 were, respectively, 3.40 (95% CI: 3.07, 3.76) and 1.71 (95% CI: 1.53, 1.92) higher risk of kidney failure when compared to A1. For each albumin category, death rate increased as albuminuria increased particularly in diabetic subjects, which was approximately 2 times higher in A3 compared to A1. Considering GFR category, it gradually increased from G1 to G4 and sharply increased from G4 to G5 in both non-diabetic and diabetic subjects. This study has quantified CKD progression in an Asian population within ordinary practice. Diabetic subjects progress through GFR and albuminuria categories and reach kidney failure about twice as rapidly as non-diabetic subjects.
关于慢性肾脏病(CKD)进展的预后信息,尤其是对于肾小球滤过率(GFR)1级和2级的情况,仍然有限。因此,开展了这项队列研究,采用竞争风险方法来确定CKD的进展情况。我们进行了一项回顾性队列研究,将泰国一个省份1997年至2011年的社区健康筛查数据与医院及死亡登记数据相联系。通过将死亡视为竞争风险因素,应用竞争风险模型来估计肾衰竭的2年、5年和10年概率以及CKD从较低GFR类别进展到较高GFR类别的中位时间。共有17074名非糖尿病CKD患者和15032名糖尿病CKD患者。糖尿病患者在不同GFR类别中的进展更快,CKD从G1进展到G2、G2进展到G3a、G3a进展到G3b、G3b进展到G4以及G4进展到G5的中位时间分别为4.4年、6.1年、4.9年、6.3年和9.0年。非糖尿病患者进展所需时间更长,相应的中位时间分别为9.4年、14.0年、11.0年、13.8年和>14.3年。在对混杂因素进行调整后,糖尿病患者发生肾衰竭的可能性比非糖尿病患者高49%(病因特异性风险比(cHR)=1.49,95%置信区间:1.37,1.62)。与A1相比,蛋白尿类别A3和A2发生肾衰竭的风险分别高3.40(95%置信区间:3.07,3.76)和1.71(95%置信区间:1.53,1.92)。对于每个蛋白尿类别,死亡率随着蛋白尿增加而升高,尤其是在糖尿病患者中,A3的死亡率相比A1大约高出2倍。考虑GFR类别,在非糖尿病和糖尿病患者中,死亡率均从G1逐渐升高至G4,并从G4急剧升高至G5。本研究对亚洲普通人群中的CKD进展情况进行了量化。糖尿病患者在GFR和蛋白尿类别方面的进展速度约为非糖尿病患者的两倍,且肾衰竭的发生速度也约为非糖尿病患者的两倍。