Boettcher Jan P, Siwakoti Yubaraj, Milojkovic Ana, Siddiqui Niyamat A, Gurung Chitra K, Rijal Suman, Das Pradeep, Kroeger Axel, Banjara Megha R
Centre for Biological Threats and Special Pathogens, Robert Koch-Institute, Nordufer 20, Berlin, 13353, Germany.
Valley College of Technical Sciences, Purbanchal University, Maharajgunj, Kathmandu, 44600, Nepal.
BMC Infect Dis. 2015 Feb 6;15:43. doi: 10.1186/s12879-015-0767-5.
To eliminate visceral leishmaniasis (VL) in India and Nepal, challenges of VL diagnosis, treatment and reporting need to be identified. Recent data indicate that VL is underreported and patients face delays when seeking treatment. Moreover, VL surveillance data might not reach health authorities on time. This study quantifies delays for VL diagnosis and treatment, and analyses the duration of VL reporting from district to central health authorities in India and Nepal.
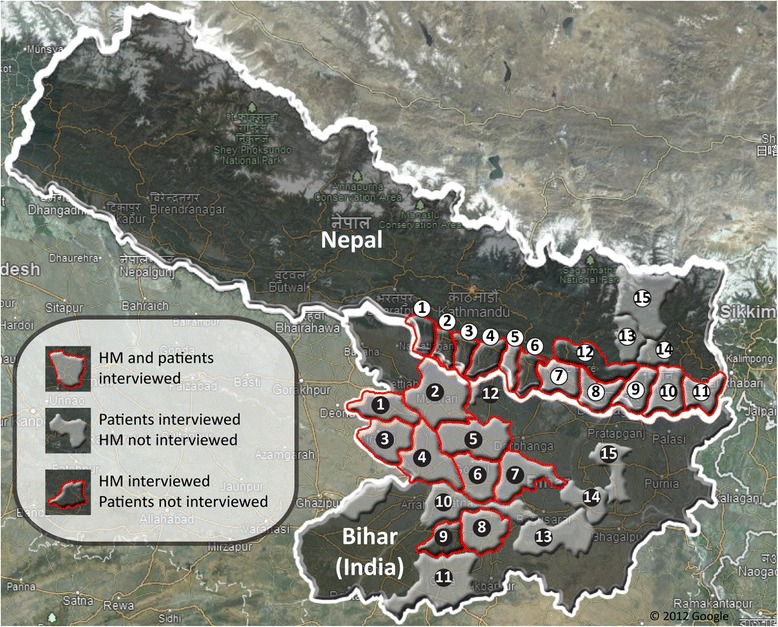
A cross-sectional study conducted in 12 districts of Terai region, Nepal, and 9 districts of Bihar State, India, in 2012. Patients were interviewed in hospitals or at home using a structured questionnaire, health managers were interviewed at their work place using a semi-structured questionnaire and in-depth interviews were conducted with central level health managers. Reporting formats were evaluated. Data was analyzed using two-tailed Mann-Whitney U or Fisher's exact test.
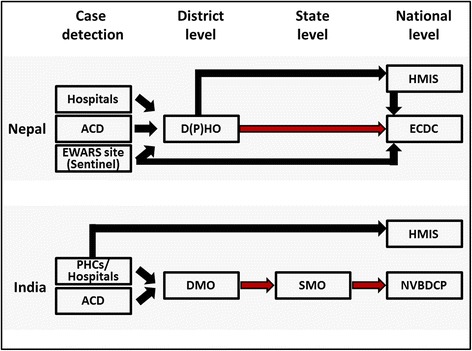
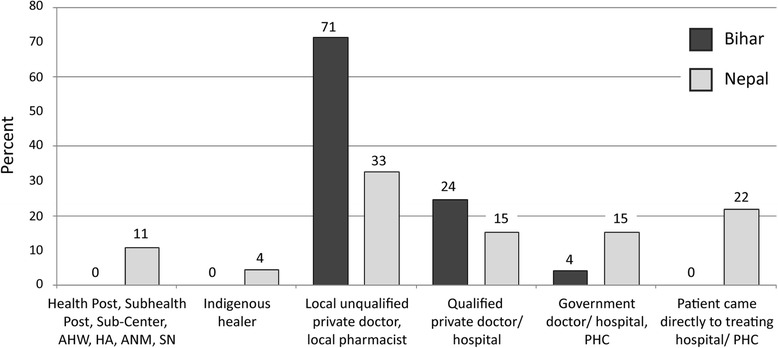
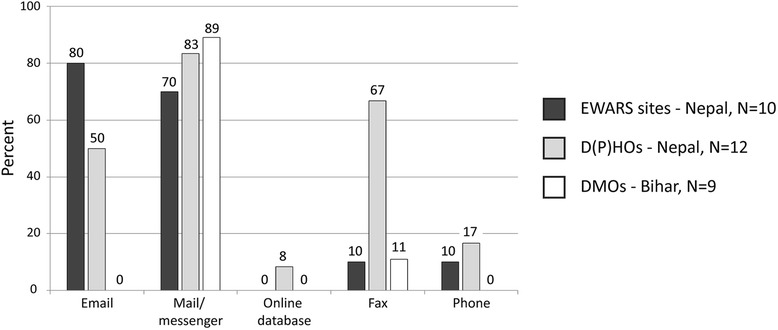
92 VL patients having experienced 103 VL episodes and 49 district health managers were interviewed. Patients waited in Nepal 30 days (CI 18-42) before seeking health care, 3.75 times longer than in Bihar (8d; CI 4-12). Conversely, the lag time from seeking health care to receiving a VL diagnosis was 3.6x longer in Bihar (90d; CI 68-113) compared to Nepal (25d; CI 13-38). The time span between diagnosis and treatment was short in both countries. VL reporting time was in Nepal 19 days for sentinel sites and 76 days for "District Public Health Offices (DPHOs)". In Bihar it was 28 days for "District Malaria Offices". In Nepal, 73% of health managers entered data into computers compared to 16% in Bihar. In both countries reporting was mainly paper based and standardized formats were rarely used.
To decrease the delay between onset of symptoms and getting a proper diagnosis and treatment the approaches in the two countries vary: In Nepal health education for seeking early treatment are needed while in Bihar the use of private and non-formal practitioners has to be discouraged. Reinforcement of VL sentinel reporting in Bihar, reorganization of DPHOs in Nepal, introduction of standardized reporting formats and electronic reporting should be conducted in both countries.
为在印度和尼泊尔消除内脏利什曼病(VL),需要明确VL诊断、治疗及报告方面存在的挑战。近期数据表明,VL存在报告不足的情况,患者在寻求治疗时会面临延误。此外,VL监测数据可能无法及时送达卫生当局。本研究对VL诊断和治疗的延误情况进行了量化,并分析了印度和尼泊尔从地区向中央卫生当局报告VL的时长。
2012年在尼泊尔特莱地区的12个区以及印度比哈尔邦的9个区开展了一项横断面研究。使用结构化问卷在医院或患者家中对患者进行访谈,使用半结构化问卷在工作场所对卫生管理人员进行访谈,并对中央级卫生管理人员进行深入访谈。对报告格式进行了评估。使用双尾曼-惠特尼U检验或费舍尔精确检验对数据进行分析。
对92例经历过103次VL发作的患者以及49名地区卫生管理人员进行了访谈。尼泊尔患者在寻求医疗服务前等待了30天(置信区间18 - 42天),比哈尔邦患者等待了8天(置信区间4 - 12天),前者等待时间是后者的3.75倍。相反,从寻求医疗服务到获得VL诊断的延迟时间,比哈尔邦(90天;置信区间68 - 113天)是尼泊尔(25天;置信区间13 - 38天)的3.6倍。两国从诊断到治疗的时间跨度都较短。尼泊尔哨点的VL报告时间为19天,“地区公共卫生办公室(DPHOs)”为76天。在比哈尔邦,“地区疟疾办公室”的报告时间为28天。在尼泊尔,73%的卫生管理人员将数据录入计算机,而在比哈尔邦这一比例为16%。两国的报告主要以纸质形式进行,很少使用标准化格式。
为减少症状出现到获得正确诊断和治疗之间的延误,两国采取的方法有所不同:在尼泊尔,需要开展关于寻求早期治疗的健康教育,而在比哈尔邦,必须不鼓励患者寻求私人和非正规从业者的帮助。两国都应加强比哈尔邦的VL哨点报告,对尼泊尔的DPHOs进行重组,引入标准化报告格式并采用电子报告。