Biais Matthieu, Ehrmann Stephan, Mari Arnaud, Conte Benjamin, Mahjoub Yazine, Desebbe Olivier, Pottecher Julien, Lakhal Karim, Benzekri-Lefevre Dalila, Molinari Nicolas, Boulain Thierry, Lefrant Jean-Yves, Muller Laurent
Crit Care. 2014 Nov 4;18(6):587. doi: 10.1186/s13054-014-0587-9.
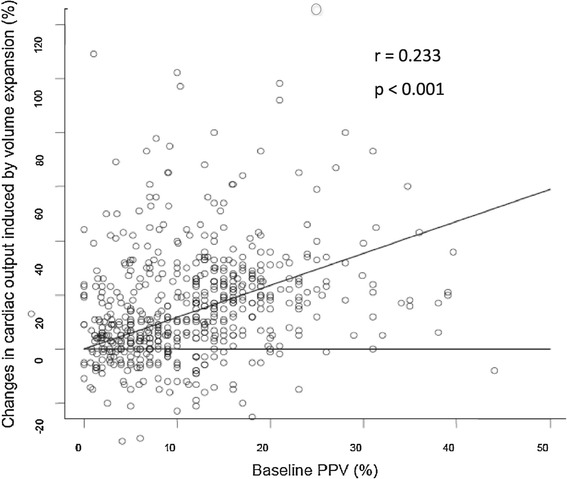
Pulse pressure variation (PPV) has been shown to predict fluid responsiveness in ventilated intensive care unit (ICU) patients. The present study was aimed at assessing the diagnostic accuracy of PPV for prediction of fluid responsiveness by using the grey zone approach in a large population.
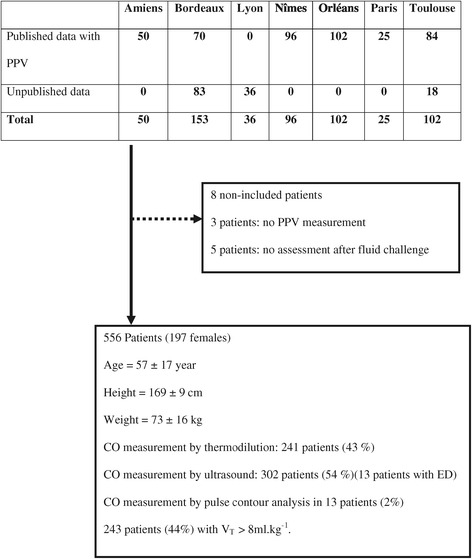
The study pooled data of 556 patients from nine French ICUs. Hemodynamic (PPV, central venous pressure (CVP) and cardiac output) and ventilator variables were recorded. Responders were defined as patients increasing their stroke volume more than or equal to 15% after fluid challenge. The receiver operating characteristic (ROC) curve and grey zone were defined for PPV. The grey zone was evaluated according to the risk of fluid infusion in hypoxemic patients.
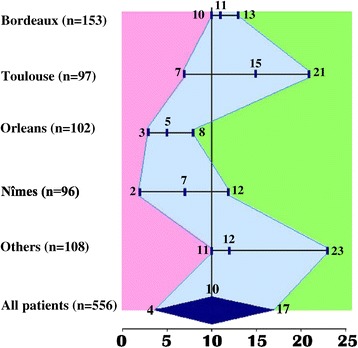
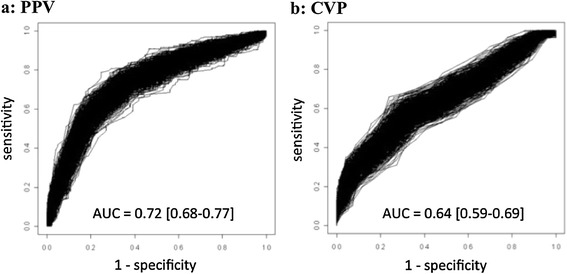
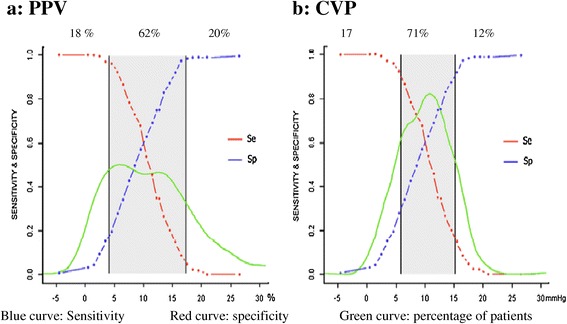
Fluid challenge led to increased stroke volume more than or equal to 15% in 267 patients (48%). The areas under the ROC curve of PPV and CVP were 0.73 (95% confidence interval (CI): 0.68 to 0.77) and 0.64 (95% CI 0.59 to 0.70), respectively (P<0.001). A grey zone of 4 to 17% (62% of patients) was found for PPV. A tidal volume more than or equal to 8 ml.kg(-1) and a driving pressure (plateau pressure - PEEP) more than 20 cmH2O significantly improved the area under the ROC curve for PPV. When taking into account the risk of fluid infusion, the grey zone for PPV was 2 to 13%.
In ventilated ICU patients, PPV values between 4 and 17%, encountered in 62% patients exhibiting validity prerequisites, did not predict fluid responsiveness.
脉压变异(PPV)已被证明可预测机械通气的重症监护病房(ICU)患者的液体反应性。本研究旨在通过在大量人群中使用灰色区域法评估PPV预测液体反应性的诊断准确性。
本研究汇总了来自9个法国ICU的556例患者的数据。记录血流动力学参数(PPV、中心静脉压(CVP)和心输出量)和呼吸机参数。反应者定义为在液体冲击后每搏量增加大于或等于15%的患者。为PPV定义了受试者工作特征(ROC)曲线和灰色区域。根据低氧血症患者液体输注的风险评估灰色区域。
267例患者(48%)在液体冲击后每搏量增加大于或等于15%。PPV和CVP的ROC曲线下面积分别为0.73(95%置信区间(CI):0.68至0.77)和0.64(95%CI 0.59至0.70)(P<0.001)。PPV的灰色区域为4%至17%(62%的患者)。潮气量大于或等于8 ml·kg⁻¹和驱动压(平台压-呼气末正压)大于20 cmH₂O显著改善了PPV的ROC曲线下面积。考虑到液体输注的风险,PPV的灰色区域为2%至13%。
在机械通气的ICU患者中,62%满足有效性前提条件的患者PPV值在4%至17%之间,不能预测液体反应性。