Make Barry J, Eriksson Göran, Calverley Peter M, Jenkins Christine R, Postma Dirkje S, Peterson Stefan, Östlund Ollie, Anzueto Antonio
Division of Pulmonary Sciences and Critical Care Medicine, National Jewish Health, University of Colorado Denver School of Medicine, Denver, CO, USA.
Department of Respiratory Medicine and Allergology, University Hospital, Lund, Sweden.
Int J Chron Obstruct Pulmon Dis. 2015 Jan 27;10:201-9. doi: 10.2147/COPD.S69589. eCollection 2015.
There is no clinically useful score to predict chronic obstructive pulmonary disease (COPD) exacerbations. We aimed to derive this by analyzing data from three existing COPD clinical trials of budesonide/formoterol, formoterol, or placebo in patients with moderate-to-very-severe COPD and a history of exacerbations in the previous year.
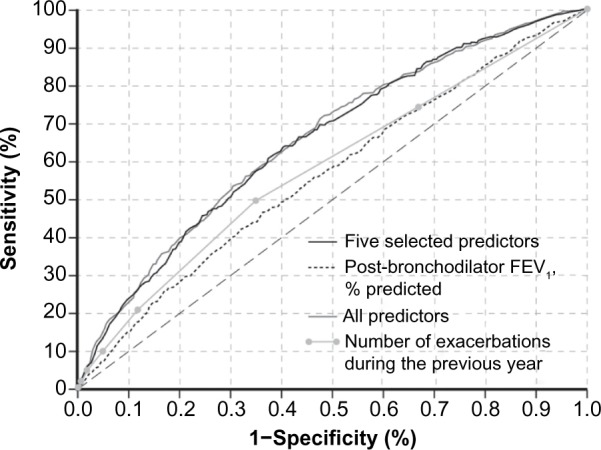
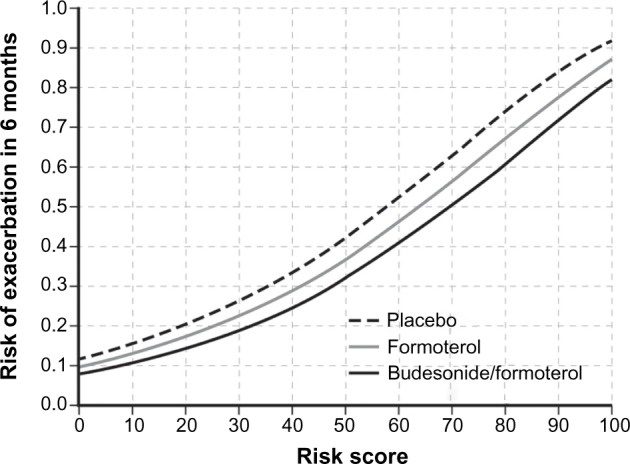
Predictive variables were selected using Cox regression for time to first severe COPD exacerbation. We determined absolute risk estimates for an exacerbation by identifying variables in a binomial model, adjusting for observation time, study, and treatment. The model was further reduced to clinically useful variables and the final regression coefficients scaled to obtain risk scores of 0-100 to predict an exacerbation within 6 months. Receiver operating characteristic (ROC) curves and the corresponding C-index were used to investigate the discriminatory properties of predictive variables.
The best predictors of an exacerbation in the next 6 months were more COPD maintenance medications prior to the trial, higher mean daily reliever use, more exacerbations during the previous year, lower forced expiratory volume in 1 second/forced vital capacity ratio, and female sex. Using these risk variables, we developed a score to predict short-term (6-month) risk of COPD exacerbations (SCOPEX). Budesonide/formoterol reduced future exacerbation risk more than formoterol or as-needed short-acting β2-agonist (salbutamol).
SCOPEX incorporates easily identifiable patient characteristics and can be readily applied in clinical practice to target therapy to reduce COPD exacerbations in patients at the highest risk.
目前尚无临床上可用于预测慢性阻塞性肺疾病(COPD)急性加重的评分系统。我们旨在通过分析三项现有COPD临床试验的数据来推导该评分系统,这三项试验分别使用布地奈德/福莫特罗、福莫特罗或安慰剂治疗中度至极重度COPD且上一年有急性加重史的患者。
使用Cox回归分析首次严重COPD急性加重的时间,以此选择预测变量。我们通过在二项模型中识别变量、调整观察时间、研究和治疗,来确定急性加重的绝对风险估计值。该模型进一步简化为临床上有用的变量,并对最终回归系数进行缩放,以获得0至100的风险评分,用于预测6个月内的急性加重情况。采用受试者工作特征(ROC)曲线及相应的C指数来研究预测变量的鉴别特性。
未来6个月内急性加重的最佳预测因素为试验前更多的COPD维持药物使用、更高的每日平均缓解药物使用量、上一年更多的急性加重次数、更低的1秒用力呼气容积/用力肺活量比值以及女性性别。利用这些风险变量,我们制定了一个预测COPD急性加重短期(6个月)风险的评分系统(SCOPEX)。与福莫特罗或按需使用的短效β2受体激动剂(沙丁胺醇)相比,布地奈德/福莫特罗能更有效地降低未来急性加重风险。
SCOPEX纳入了易于识别的患者特征,可在临床实践中轻松应用,以针对高危患者进行治疗,从而减少COPD急性加重。