McCammack Kevin C, Sadler Charlotte, Guo Yueyang, Ramaswamy Raja S, Farid Nikdokht
University of California, San Diego, Department of Radiology, San Diego, California.
University of California, San Diego, Department of Emergency Medicine, San Diego, California.
West J Emerg Med. 2015 Jan;16(1):43-9. doi: 10.5811/westjem.2014.10.19488. Epub 2014 Dec 1.
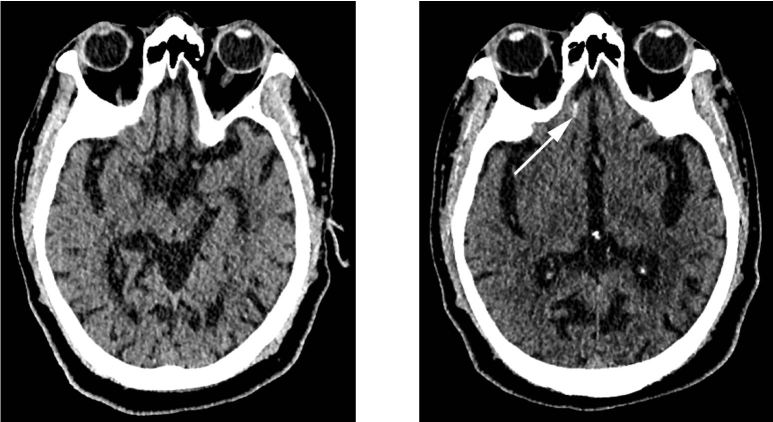
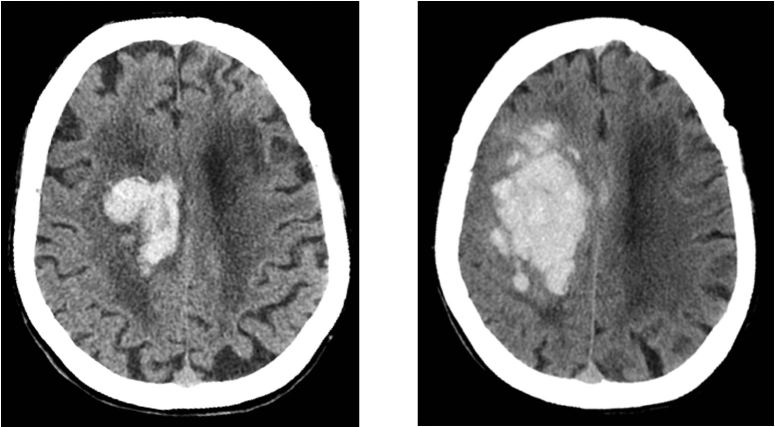
Evaluation recommendations for patients on anticoagulant and antiplatelet (ACAP) therapy that present after mild traumatic brain injury (TBI) are controversial. At our institution, an initial noncontrast head computed tomography (HCT) is performed, with a subsequent HCT performed six hours later to exclude delayed intracranial hemorrhage (ICH). This study was performed to evaluate the yield and advisability of this approach.
We performed a retrospective review of subjects undergoing evaluation for ICH after mild TBI in patients on ACAP therapy between January of 2012 and April of 2013. We assessed for the frequency of ICH on both the initial noncontrast HCT and on the routine six-hour follow-up HCT. Additionally, chart review was performed to evaluate the clinical implications of ICH, when present, and to interrogate whether pertinent clinical and laboratory data may predict the presence of ICH prior to imaging. We used multivariate generalized linear models to assess whether presenting Glasgow Coma Score (GCS), loss of consciousness (LOC), neurological or physical examination findings, international normalized ratio, prothrombin time, partial thromboplastin time, platelet count, or specific ACAP regimen predicted ICH.
144 patients satisfied inclusion criteria. Ten patients demonstrated initial HCT positive for ICH, with only one demonstrating delayed ICH on the six-hour follow-up HCT. This patient was discharged without any intervention required or functional impairment. Presenting GCS deviation (p<0.001), LOC (p=0.04), neurological examination findings (p<0.001), clopidogrel (p=0.003), aspirin (p=0.03) or combination regimen (p=0.004) use were more commonly seen in patients with ICH.
Routine six-hour follow-up HCT is likely not indicated in patients on ACAP therapy, as our study suggests clinically significant delayed ICH does not occur. Additionally, presenting GCS deviation, LOC, neurological examination findings, clopidogrel, aspirin or combination regimen use may predict ICH, and, in the absence of these findings, HCT may potentially be forgone altogether.
对于轻度创伤性脑损伤(TBI)后接受抗凝和抗血小板(ACAP)治疗的患者,评估建议存在争议。在我们机构,首先进行一次头部非增强计算机断层扫描(HCT),随后在六小时后再进行一次HCT以排除迟发性颅内出血(ICH)。本研究旨在评估这种方法的检出率及合理性。
我们对2012年1月至2013年4月期间接受ACAP治疗且因轻度TBI接受ICH评估的患者进行了回顾性研究。我们评估了初次头部非增强HCT及常规六小时随访HCT上ICH的发生频率。此外,查阅病历以评估ICH出现时的临床意义,并探究相关临床和实验室数据在影像学检查前是否可预测ICH的存在。我们使用多变量广义线性模型评估就诊时的格拉斯哥昏迷评分(GCS)、意识丧失(LOC)、神经或体格检查结果、国际标准化比值、凝血酶原时间、活化部分凝血活酶时间、血小板计数或特定ACAP治疗方案是否可预测ICH。
144例患者符合纳入标准。10例患者初次HCT显示ICH阳性,仅1例在六小时随访HCT时显示迟发性ICH。该患者未经任何干预即出院,且无功能障碍。就诊时GCS偏差(p<0.001)、LOC(p= 0.04)、神经检查结果(p<0.001)、使用氯吡格雷(p=0.003)、阿司匹林(p=0.03)或联合治疗方案(p=0.004)在ICH患者中更为常见。
对于接受ACAP治疗的患者,可能无需进行常规六小时随访HCT,因为我们的研究表明临床上不会出现有显著意义的迟发性ICH。此外,就诊时GCS偏差、LOC、神经检查结果、使用氯吡格雷、阿司匹林或联合治疗方案可能预测ICH,若无这些表现,可能完全无需进行HCT检查。