Ranzani Otavio T, Simpson Evelyn Senna, Augusto Talita Barbosa, Cappi Sylas Bezerra, Noritomi Danilo Teixeira
Crit Care. 2014 Oct 24;18(5):580. doi: 10.1186/s13054-014-0580-3.
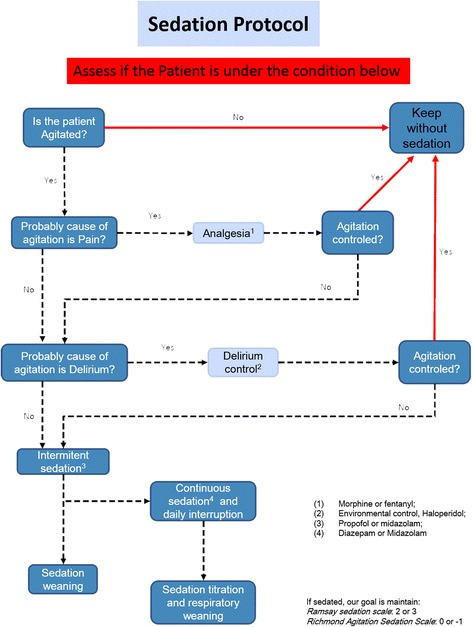
Oversedation frequently occurs in ICUs. We aimed to evaluate a minimal sedation policy, using sedative consumption as a monitoring tool, in a network of ICUs targeting decrement of oversedation and mechanical ventilation (MV) duration.
A prospective quality improvement project was conducted in ten ICUs within a network of nonteaching hospitals in Brazil during a 2-year period (2010 to 2012). In the first 12 months (the preintervention period), we conducted an audit to identify sedation practice and barriers to current guideline-based practice regarding sedation. In the postintervention period, we implemented a multifaceted program, including multidisciplinary daily rounds, and monthly audits focusing on sedative consumption, feedback and benchmarking purposes. To analyze the effect of the campaign, we fit an interrupted time series (ITS). To account for variability among the network ICUs, we fit a hierarchical model.
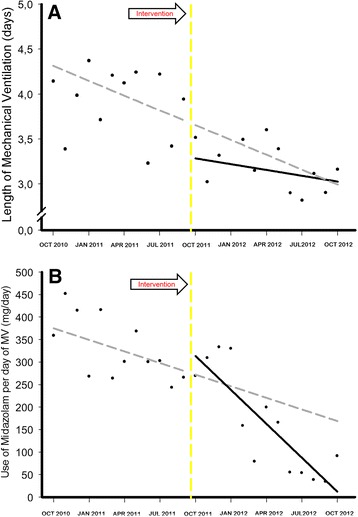
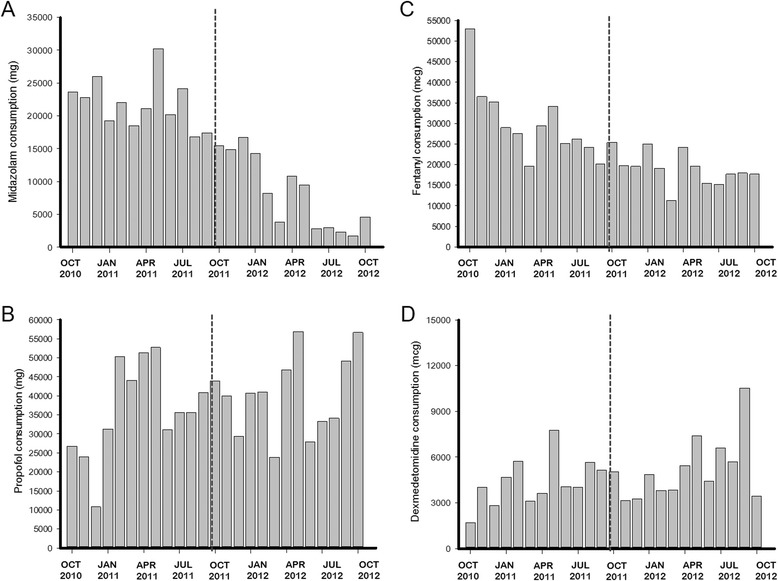
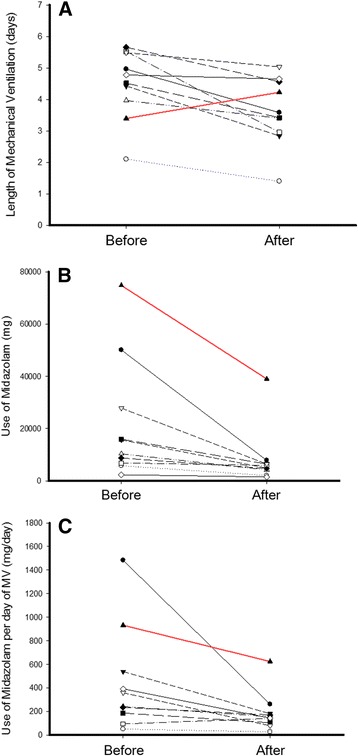
During the study period, 21% of patients received MV (4,851/22,963). In the postintervention period, the length of MV was lower (3.91 ± 6.2 days versus 3.15 ± 4.6 days; mean difference, -0.76 (95% CI, -1.10; -0.43), P <0.001) and 28 ventilator-free days were higher (16.07 ± 12.2 days versus 18.33 ± 11.6 days; mean difference, 2.30 (95% CI, 1.57; 3.00), P <0.001) than in the preintervention period. Midazolam consumption (in milligrams per day of MV) decreased from 329 ± 70 mg/day to 163 ± 115 mg/day (mean difference, -167 (95% CI, -246; -87), P <0.001). In contrast, consumption of propofol (P = 0.007), dexmedetomidine (P = 0.017) and haloperidol (P = 0.002) increased in the postintervention period, without changes in the consumption of fentanyl. Through ITS, age (P = 0.574) and Simplified Acute Physiology Score III (P = 0.176) remained stable. The length of MV showed a secular effect (secular trend β(1) = -0.055, P = 0.012) and a strong decrease immediately after the intervention (intervention β(2) = -0.976, P <0.001). The impact was maintained over the course of one year, despite the waning trend for the intervention's effect (postintervention trend β(3)= 0.039, P = 0.095).
By using a light sedation policy in a group of nonteaching hospitals, we reproduced the benefits that have previously been demonstrated in controlled settings. Furthermore, systematic monitoring of sedative consumption should be a feasible instrument for supporting the implementation of a protocol on a large scale.
在重症监护病房(ICU)中,过度镇静经常发生。我们旨在评估一种以镇静药物消耗量作为监测工具的最小化镇静策略,该策略应用于一个旨在减少过度镇静和机械通气(MV)时长的ICU网络中。
在巴西非教学医院网络中的10个ICU开展了一项为期2年(2010年至2012年)的前瞻性质量改进项目。在最初的12个月(干预前期),我们进行了一次审核,以确定镇静实践以及当前基于指南的镇静实践所面临的障碍。在干预后期,我们实施了一个多方面的项目,包括多学科每日查房,以及以镇静药物消耗量、反馈和基准化为重点的月度审核。为分析该活动的效果,我们采用了中断时间序列(ITS)。为考虑网络内各ICU之间的差异,我们采用了分层模型。
在研究期间,21%的患者接受了MV(4851/22963)。在干预后期,MV时长缩短(分别为3.91±6.2天和3.15±4.6天;平均差值为-0.76(95%CI,-1.10;-0.43),P<0.001),无呼吸机天数增加(分别为16.07±12.2天和18.33±11.6天;平均差值为2.30(95%CI,1.57;3.00),P<0.001)。咪达唑仑消耗量(以MV每日毫克数计)从329±70毫克/天降至163±115毫克/天(平均差值为-167(95%CI,-246;-87),P<0.001)。相比之下,在干预后期丙泊酚(P=0.007)、右美托咪定(P=0.017)和氟哌啶醇(P=0.002)的消耗量增加,而芬太尼的消耗量无变化。通过ITS分析,年龄(P=0.574)和简化急性生理学评分III(P=0.176)保持稳定。MV时长呈现长期效应(长期趋势β(1)=-0.055,P=0.012),且在干预后立即大幅下降(干预β(2)=-0.976,P<0.001)。尽管干预效果呈减弱趋势(干预后趋势β(3)=0.039,P=0.095),但这种影响在一年中持续存在。
通过在一组非教学医院中采用轻度镇静策略,我们再现了先前在对照环境中所证明的益处。此外,系统监测镇静药物消耗量应是支持大规模实施方案的可行手段。