Thaker Nikhil G, Hoffman Karen E, Stauder Michael C, Shaitelman Simona F, Strom Eric A, Tereffe Welela, Smith Benjamin D, Perkins George H, Huo Lei, Munsell Mark F, Pusztai Lajos, Buchholz Thomas A, Woodward Wendy A
Department of Radiation Oncology, Unit 1202, The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, TX 77030 USA.
Department of Pathology, The University of Texas MD Anderson Cancer Center, Houston, TX USA.
Springerplus. 2015 Jan 30;4:36. doi: 10.1186/s40064-015-0840-y. eCollection 2015.
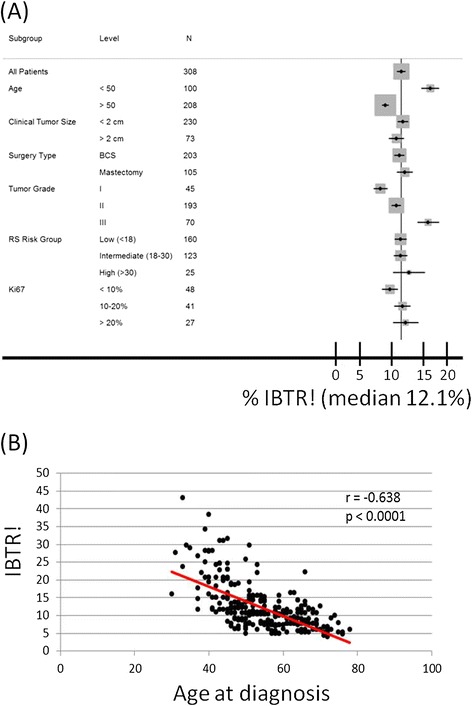
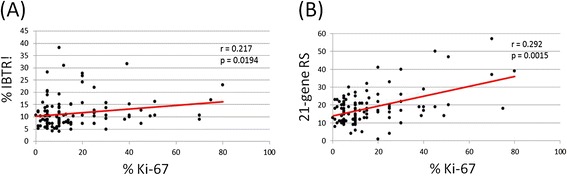
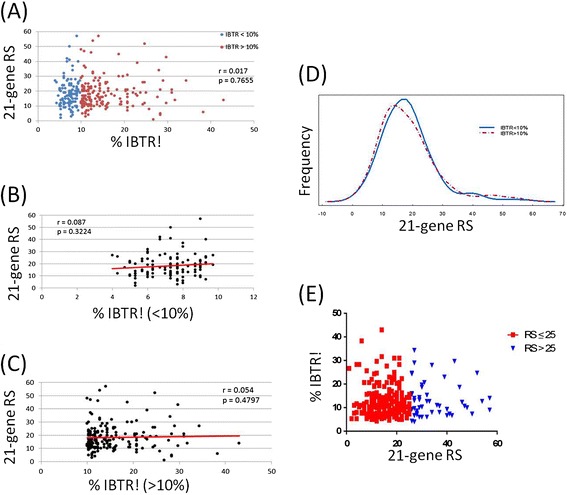
Clinicians have traditionally used clinicopathological (CP) factors to determine locoregional recurrence (LR) risk of breast cancer and have generated the IBTR! nomogram to predict the risk of ipsilateral breast tumor recurrence (IBTR). The 21-gene recurrence score (RS) assay was recently correlated with LR in retrospective studies. The objective of this study was to examine the relationship between the RS and IBTR!. CP characteristics of 308 consecutive patients who underwent RS testing at our institution were examined. IBTR! was used to estimate the risk of 10-year IBTR. Descriptive statistics were used to compare the RS with the estimated IBTR!. Given a low event rate in this cohort, actual IBTR rates were not reported. Most patients had stage I/II (98%) and grade I/II (77%) disease. Median age was 54 years (range, 30-78). Median IBTR! without radiation therapy was 10% (mean, 12% [range, 4-43%]). RS was low (<18), intermediate (18-30), and high (>30) in 52% (n = 160), 40% (n = 123), and 8% (n = 25) patients. Overall, IBTR! did not correlate with RS (P = .77). We saw no correlation between RS and IBTR! in patients with less than (P = .32) or greater than (P = .48) a 10% risk of IBTR. Interestingly, Ki-67 expression correlated with both IBTR! (P = .019) and the RS (P = .002). Further study is warranted to determine if the RS can provide complementary biological information to CP factors in estimating the risk of LR. Prospective studies evaluating this association may potentially allow for individualized treatment decisions.
传统上,临床医生使用临床病理(CP)因素来确定乳腺癌的局部区域复发(LR)风险,并生成了IBTR!列线图来预测同侧乳腺肿瘤复发(IBTR)的风险。在回顾性研究中,21基因复发评分(RS)检测最近与LR相关。本研究的目的是探讨RS与IBTR!之间的关系。对在我们机构接受RS检测的308例连续患者的CP特征进行了检查。IBTR!用于估计10年IBTR的风险。使用描述性统计来比较RS与估计的IBTR!。鉴于该队列中的事件发生率较低,未报告实际的IBTR率。大多数患者患有I/II期(98%)和I/II级(77%)疾病。中位年龄为54岁(范围30-78岁)。未接受放疗的患者中位IBTR!为10%(平均12%[范围4-43%])。52%(n = 160)、40%(n = 123)和8%(n = 25)的患者RS较低(<18)、中等(18-30)和较高(>30)。总体而言,IBTR!与RS无相关性(P = 0.77)。在IBTR风险低于10%(P = 0.32)或高于10%(P = 0.48)的患者中,我们未发现RS与IBTR!之间存在相关性。有趣的是,Ki-67表达与IBTR!(P = 0.019)和RS(P = 0.002)均相关。有必要进行进一步研究以确定RS在估计LR风险时是否可以为CP因素提供补充生物学信息。评估这种关联的前瞻性研究可能会允许做出个性化的治疗决策。