Wells Philip S, Gebel Martin, Prins Martin H, Davidson Bruce L, Lensing Anthonie Wa
Department of Medicine, University of Ottawa, Ottawa Hospital Research Institute, Ottawa, Canada.
Bayer HealthCare, Wuppertal, Germany.
Thromb J. 2014 Nov 26;12:26. doi: 10.1186/1477-9560-12-26. eCollection 2014.
Statins may reduce the risk of first and recurrent venous thromboembolism (VTE). No data are available on their potential benefit in patients treated with the oral anticoagulant rivaroxaban.
The EINSTEIN DVT/PE and EINSTEIN Extension studies compared rivaroxaban with standard of care (n=8280) and placebo (n=1188), respectively. The incidences of recurrent VTE and major bleeding per 100 patient-years for exposure (or not) to statins were calculated. A Cox proportional hazards model was constructed, stratified by index event and intended treatment duration, with statin use as a time-dependent variable, for each treatment group (rivaroxaban vs enoxaparin/vitamin K antagonist or placebo) and adjusted for relevant variables.
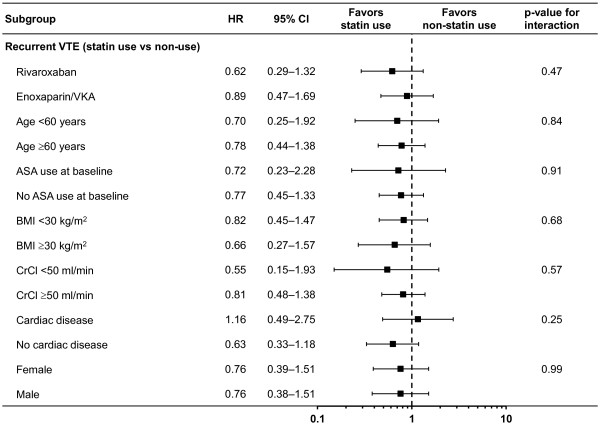
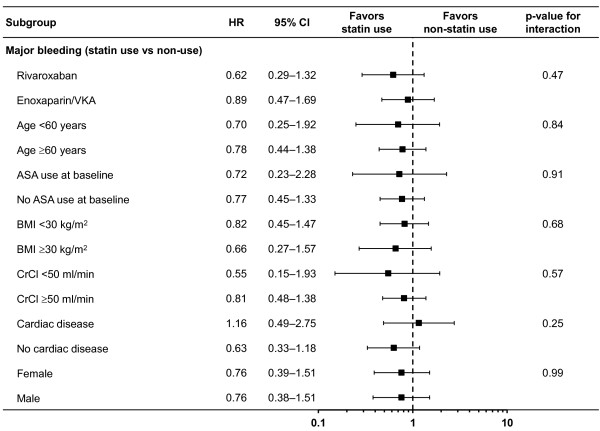
In EINSTEIN DVT/PE, 1509 (18.3%) patients used statins during the at-risk period, and 6731 (81.7%) did not. Overall, 2.6 recurrent VTEs occurred per 100 patient-years with statin use compared with 3.8 per 100 patient-years without statins (adjusted hazard ratio [HR] 0.76; 95% confidence interval [CI] 0.46-1.25). HRs for recurrent VTE were similar for concomitant use of rivaroxaban-statin and enoxaparin/VKA-statin. Major bleeding events occurred in 3.0 per 100 patient-years with statin use compared with 2.3 per 100 patient-years without statins (adjusted HR 0.77; 95% CI 0.46-1.29). Due to adjustments in the Cox regression model, the direction of this HR is in contrast to the crude comparison. In EINSTEIN Extension, no recurrent VTEs occurred with statin use in the rivaroxaban group compared with 1.6 per 100 patient-years without statins. In the placebo group, 12.2 recurrent VTEs occurred per 100 patient-years with statin use compared with 13.2 per 100 patient-years without (adjusted HR 0.81; 95% CI 0.35-1.86).
The effect of statins in this secondary analysis of the EINSTEIN VTE treatment program is consistent with other studies that suggest a reduced risk of recurrent VTE, but conclusive evidence of this benefit is lacking. Statins are simple to use, inexpensive, very safe and do not cause bleeding. Therefore, the potential effect on reducing recurrent VTE, which is in the range of that of acetylsalicylic acid, deserves evaluation in a large randomized trial.
ClinicalTrials.gov: EINSTEIN PE, NCT00439777; EINSTEIN DVT, NCT00440193; EINSTEIN Extension, NCT00439725.
他汀类药物可能降低首次及复发性静脉血栓栓塞(VTE)的风险。关于其在接受口服抗凝药利伐沙班治疗的患者中的潜在益处,目前尚无相关数据。
EINSTEIN DVT/PE研究和EINSTEIN扩展研究分别将利伐沙班与标准治疗(n = 8280)及安慰剂(n = 1188)进行了比较。计算了他汀类药物暴露(或未暴露)情况下每100患者年复发性VTE和大出血的发生率。针对每个治疗组(利伐沙班对比依诺肝素/维生素K拮抗剂或安慰剂),构建了Cox比例风险模型,按指数事件和预期治疗时长进行分层,将他汀类药物的使用作为时间依赖性变量,并对相关变量进行了调整。
在EINSTEIN DVT/PE研究中,1509名(18.3%)患者在风险期使用了他汀类药物,6731名(81.7%)未使用。总体而言,使用他汀类药物的患者每100患者年发生2.6次复发性VTE,未使用他汀类药物的患者为每100患者年3.8次(调整后风险比[HR] 0.76;95%置信区间[CI] 0.46 - 1.25)。利伐沙班 - 他汀类药物联合使用与依诺肝素/维生素K拮抗剂 - 他汀类药物联合使用时复发性VTE的HR相似。使用他汀类药物的患者每100患者年发生3.0次大出血事件,未使用他汀类药物的患者为每100患者年2.3次(调整后HR 0.77;95% CI 0.46 - 1.29)。由于Cox回归模型中的调整,该HR的方向与粗略比较结果相反。在EINSTEIN扩展研究中,利伐沙班组使用他汀类药物未发生复发性VTE,未使用他汀类药物的患者每100患者年发生1.6次。在安慰剂组中,使用他汀类药物的患者每100患者年发生12.2次复发性VTE,未使用的患者为每100患者年13.2次(调整后HR 0.81;95% CI 0.35 - 1.86)。
在EINSTEIN VTE治疗项目的这项二次分析中,他汀类药物的作用与其他研究一致,提示复发性VTE风险降低,但缺乏该益处的确凿证据。他汀类药物使用简便、价格低廉、非常安全且不会引起出血。因此,其在降低复发性VTE方面的潜在作用(与阿司匹林的作用范围相当)值得在大型随机试验中进行评估。
ClinicalTrials.gov:EINSTEIN PE,NCT00439777;EINSTEIN DVT,NCT00440193;EINSTEIN扩展,NCT004