Ilunga-Ilunga Félicien, Levêque Alain, Ngongo Léon Okenge, Laokri Samia, Dramaix Michèle
Institut Supérieur des Techniques Médicales de Kinshasa , RD Congo ; Université Libre de Bruxelles, School of Public Health, Research Centre in Epidemiology, Biostatistics and Clinical Research , Brussels, Belgium.
Université Libre de Bruxelles, School of Public Health, Research Centre in Epidemiology, Biostatistics and Clinical Research , Brussels, Belgium.
Trop Med Health. 2015 Mar;43(1):11-9. doi: 10.2149/tmh.2014-19. Epub 2014 Oct 16.
In the Democratic Republic of Congo (DRC), few studies have focused on treatment-seeking paths selected by caretakers for the management of severe childhood malaria in an urban environment. The present study aims at describing the treatment-seeking paths according to the characteristics of households, as well as the subsequent impact on pre-hospitalisation delay and malarial fatality and on the main syndromes associated with severe childhood malaria.
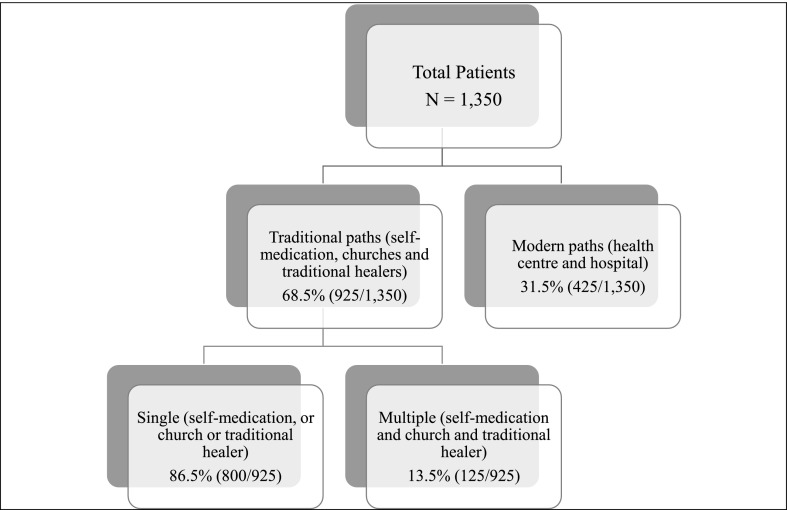
This descriptive study included data collected at nine hospitals in Kinshasa between January and November 2011. A total of 1,350 children, under 15 years of age and hospitalised for severe malaria, were included in the study.
Regarding the management of malaria, 31.5% of households went directly to the health centre or hospital while 68.5% opted for self-medication, church and/or traditional healing therapy. The most frequent first-line option was self-medication, adopted by more than 61.5% of households. Nevertheless, rational self-medication using antimalarial drugs recommended by the WHO (artemisinin-based combinations) was reported for only 5.5% of children. Only 12.5% of households combined 2 or 3 traditional options. The following criteria influenced the choice of a modern vs. traditional path: household socioeconomic level, residential environment, maternal education level and religious beliefs. When caretakers opted for traditional healing therapy, the pre-hospitalisation delay was longer and the occurrence of respiratory distress, severe anaemia and mortality was higher.
The implementation of a malaria action plan in the Democratic Republic of Congo should take into account the diversity and pluralistic character of treatment-seeking behaviours in order to promote the most appropriate options (hospital and rational self-medication) and to avoid detrimental outcomes.
在刚果民主共和国(DRC),很少有研究关注城市环境中照顾者为管理儿童重症疟疾而选择的就医途径。本研究旨在根据家庭特征描述就医途径,以及其对住院前延误、疟疾死亡和与儿童重症疟疾相关的主要综合征的后续影响。
这项描述性研究纳入了2011年1月至11月在金沙萨九家医院收集的数据。共有1350名15岁以下因重症疟疾住院的儿童纳入研究。
关于疟疾的管理,31.5%的家庭直接前往健康中心或医院,而68.5%选择自我用药、求助教会和/或传统治疗方法。最常见的一线选择是自我用药,超过61.5%的家庭采用。然而,据报告只有5.5%的儿童使用了世界卫生组织推荐的抗疟药物(以青蒿素为基础的复方制剂)进行合理的自我用药。只有12.5%的家庭结合了2种或3种传统方法。以下标准影响了现代就医途径与传统就医途径的选择:家庭社会经济水平、居住环境、母亲教育水平和宗教信仰。当照顾者选择传统治疗方法时,住院前延误更长,呼吸窘迫、严重贫血和死亡率的发生率更高。
刚果民主共和国疟疾行动计划的实施应考虑就医行为的多样性和多元性,以推广最合适的选择(住院和合理的自我用药),避免有害后果。