Koffi Alain K, Kalter Henry D, Loveth Ezenwa N, Quinley John, Monehin Joseph, Black Robert E
Institute for International Programs/ Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, United States of America.
National Population Commission, Abuja, Nigeria.
PLoS One. 2017 May 31;12(5):e0177025. doi: 10.1371/journal.pone.0177025. eCollection 2017.
Millions of children worldwide suffer and die from conditions for which effective interventions exist. While there is ample evidence regarding these diseases, there is a dearth of information on the social factors associated with child mortality.
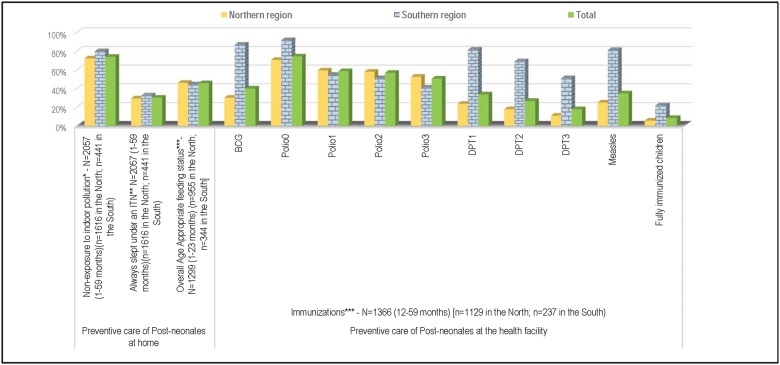
The 2014 Verbal and Social Autopsy Study was conducted based on a nationally representative sample of 3,254 deaths that occurred in children under the age of five and were reported on the birth history component of the 2013 Nigerian Demographic and Health Survey. We conducted a descriptive analysis of the preventive and curative care sought and obtained for the 2,057 children aged 1-59 months who died in Nigeria and performed regional (North vs. South) comparisons.
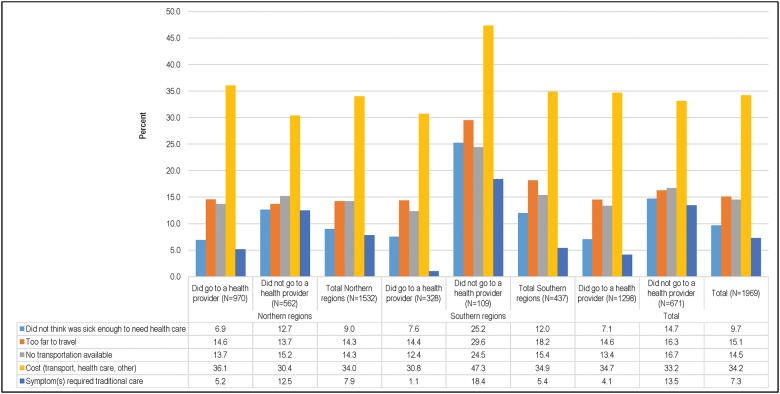
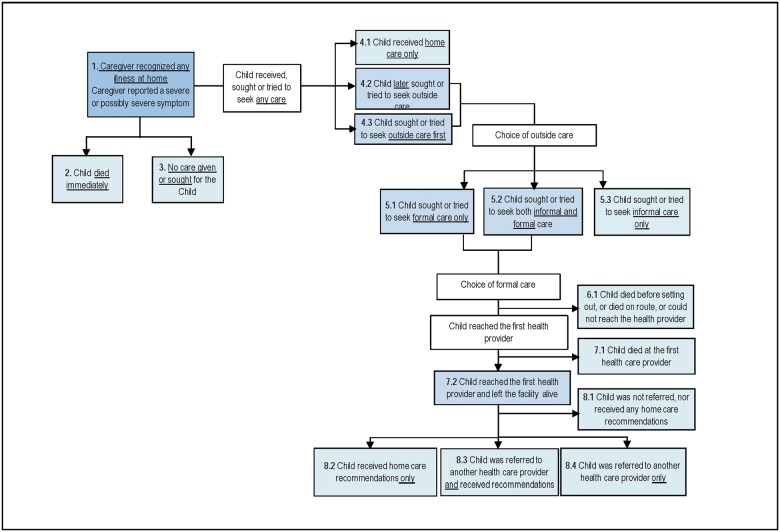
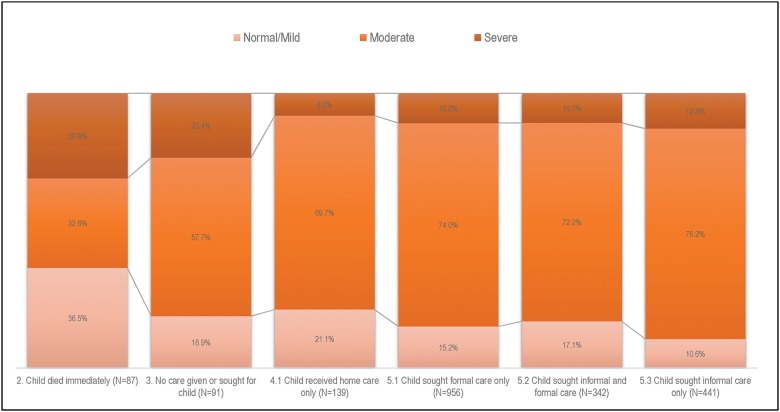
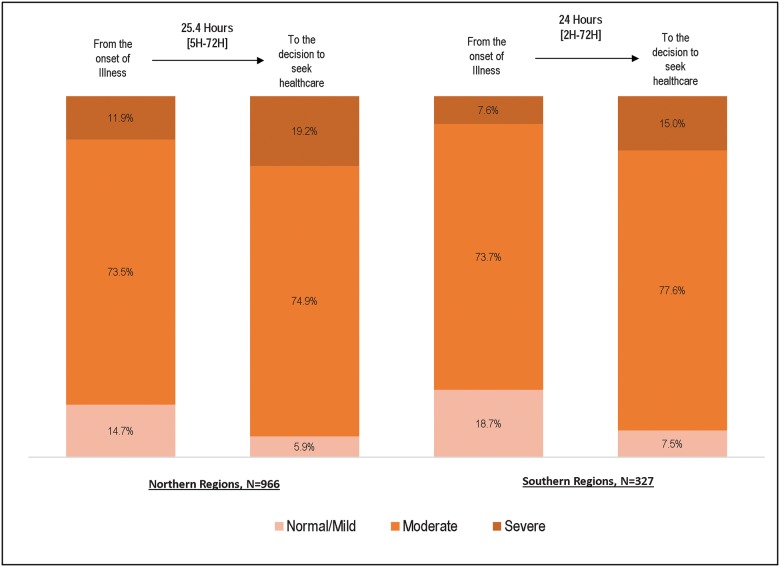
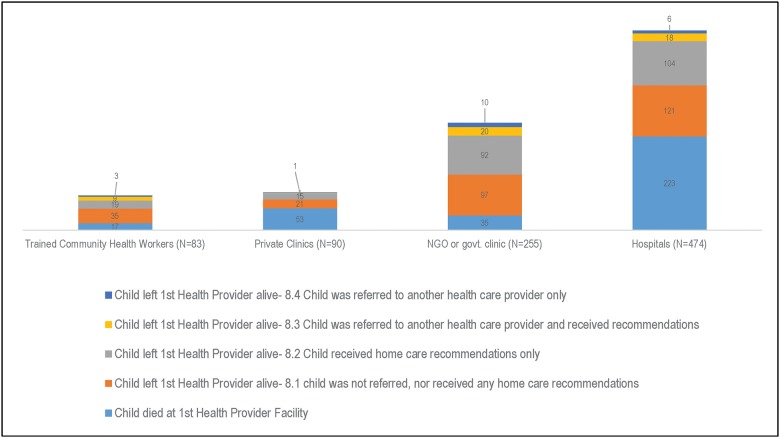
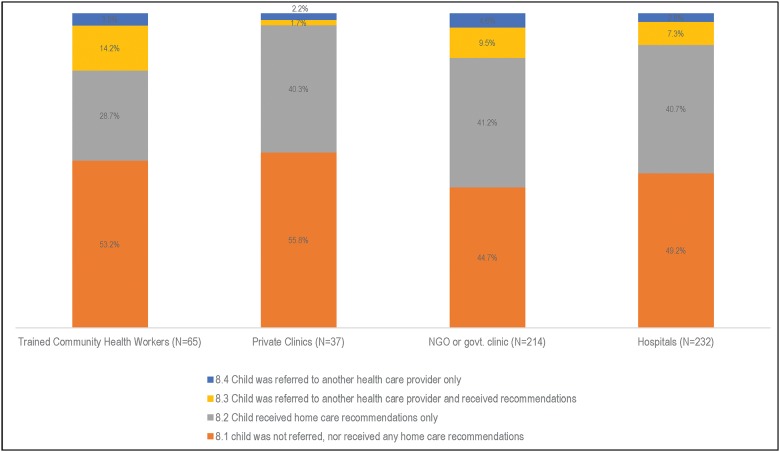
A total of 1,616 children died in the northern region, while 441 children died in the South. The majority (72.5%) of deceased children in the northern region were born to mothers who had no education, married at a young age, and lived in the poorest two quintiles of households. When caregivers first noticed that their child was ill, a median of 2 days passed before they sought or attempted to seek healthcare for their children. The proportion of children who reached and departed from their first formal healthcare provider alive was greater in the North (30.6%) than in the South (17.9%) (p<0.001). A total of 548 children were moderately or severely sick at discharge from the first healthcare provider, yet only 3.9%-18.1% were referred to a second healthcare provider. Cost, lack of transportation, and distance from healthcare facilities were the most commonly reported barriers to formal care-seeking behavior.
Maternal, household, and healthcare system factors contributed to child mortality in Nigeria. Information regarding modifiable social factors may be useful in planning intervention programs to promote child survival in Nigeria and other low-income countries in sub-Saharan Africa.
全球数以百万计的儿童正遭受一些疾病的折磨甚至死亡,而针对这些疾病存在有效的干预措施。虽然关于这些疾病有充分的证据,但缺乏与儿童死亡率相关的社会因素方面的信息。
2014年言语和社会死因调查研究基于2013年尼日利亚人口与健康调查出生史部分报告的3254例5岁以下儿童死亡的全国代表性样本进行。我们对尼日利亚1至59个月死亡的2057名儿童寻求和获得的预防及治疗护理进行了描述性分析,并进行了区域(北部与南部)比较。
北部地区共有1616名儿童死亡,南部有441名儿童死亡。北部地区大多数(72.5%)死亡儿童的母亲未受过教育、早婚且生活在最贫困的两个五分位家庭。当照料者首次注意到孩子生病时,中位数为2天后他们才为孩子寻求或试图寻求医疗保健。首次正式医疗保健提供者处存活到达和离开的儿童比例在北部(30.6%)高于南部(17.9%)(p<0.001)。共有548名儿童在首次医疗保健提供者处出院时病情为中度或重度,但只有3.9%-18.1%被转诊至二级医疗保健提供者。费用、缺乏交通工具以及距离医疗设施远是最常报告的寻求正规医疗行为的障碍。
母亲、家庭和医疗保健系统因素导致了尼日利亚的儿童死亡。关于可改变的社会因素的信息可能有助于规划干预项目,以促进尼日利亚及撒哈拉以南非洲其他低收入国家的儿童生存。