Helmschrott Matthias, Rivinius Rasmus, Ruhparwar Arjang, Schmack Bastian, Erbel Christian, Gleissner Christian A, Akhavanpoor Mohammadreza, Frankenstein Lutz, Ehlermann Philipp, Bruckner Tom, Katus Hugo A, Doesch Andreas O
Department of Cardiology, Angiology, Pneumology, University of Heidelberg, Heidelberg, Germany.
Department of Cardiac Surgery, University of Heidelberg, Heidelberg, Germany.
Drug Des Devel Ther. 2015 Feb 24;9:1217-24. doi: 10.2147/DDDT.S79343. eCollection 2015.
Nephrotoxicity is a serious adverse effect of calcineurin inhibitor therapy in patients after heart transplantation (HTX).
In this retrospective registry study, renal function within the first 2 years after HTX in patients receiving de novo calcineurin inhibitor treatment, that is, cyclosporine A (CSA) or tacrolimus (TAC), was analyzed. In a consecutive subgroup analysis, renal function in patients receiving conventional tacrolimus (CTAC) was compared with that of patients receiving extended-release tacrolimus (ETAC).
Data from 150 HTX patients at Heidelberg Heart Transplantation Center were retrospectively analyzed. All patients were continuously receiving the primarily applied calcineurin inhibitor during the first 2 years after HTX and received follow-up care according to center practice.
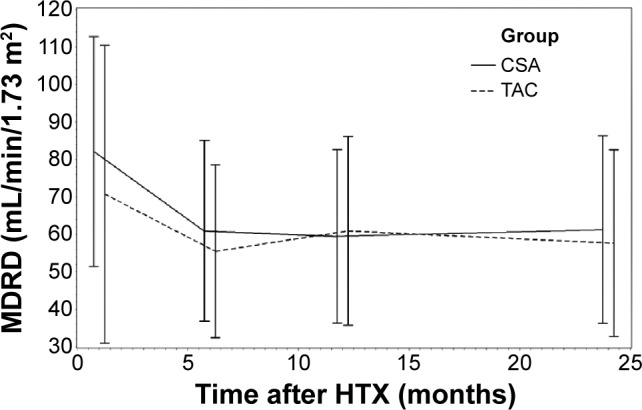
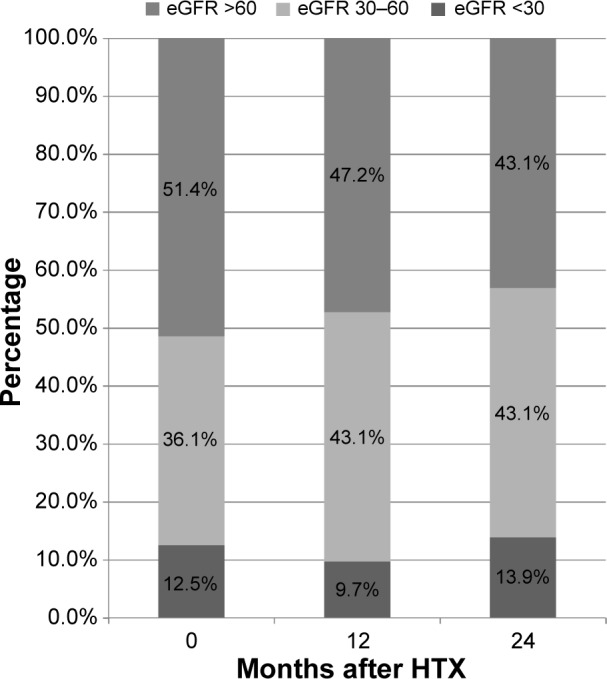
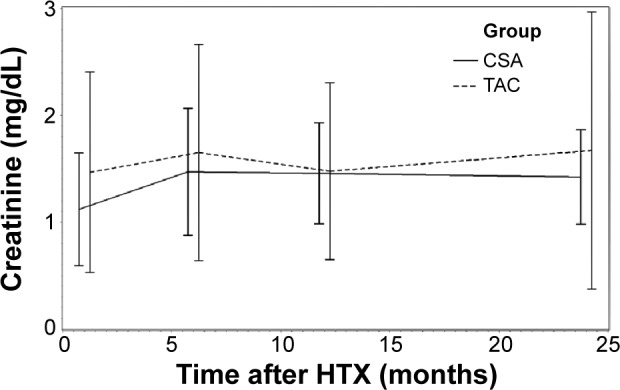
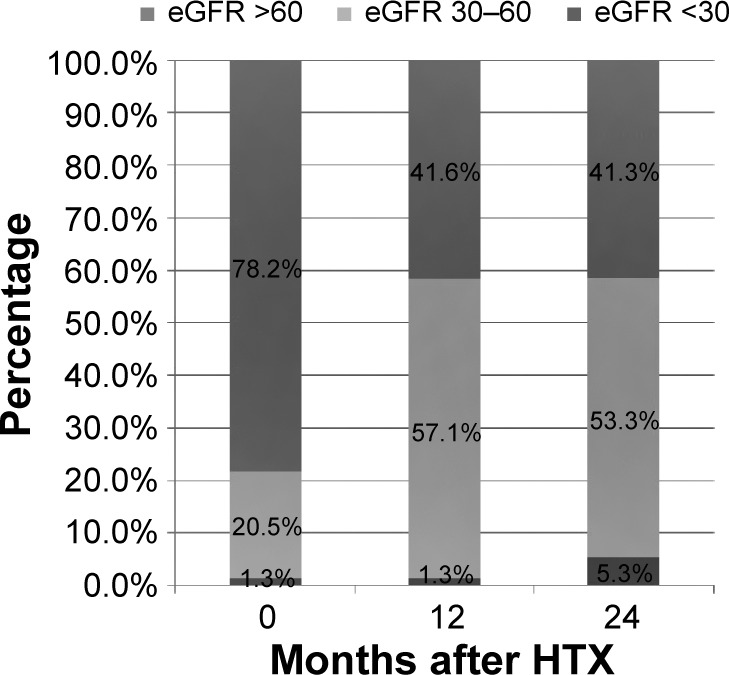
Within the first 2 years after HTX, serum creatinine increased significantly in patients receiving CSA (P<0.0001), whereas in patients receiving TAC, change of serum creatinine was not statistically significant (P=not statistically significant [ns]). McNemar's test detected a significant accumulation of patients with deterioration of renal function in the first half year after HTX among patients receiving CSA (P=0.0004). In patients receiving TAC, no significant accumulation of patients with deterioration of renal function during the first 2 years after HTX was detectable (all P=ns). Direct comparison of patients receiving CTAC versus those receiving ETAC detected no significant differences regarding renal function between patients primarily receiving CTAC or ETAC treatment during study period (all P=ns).
CSA is associated with a more pronounced deterioration of renal function, especially in the first 6 months after HTX, in comparison with patients receiving TAC as baseline immunosuppressive therapy.
肾毒性是心脏移植(HTX)患者接受钙调神经磷酸酶抑制剂治疗的严重不良反应。
在这项回顾性登记研究中,分析了接受初始钙调神经磷酸酶抑制剂治疗(即环孢素A(CSA)或他克莫司(TAC))的HTX患者在HTX后前2年内的肾功能。在连续亚组分析中,比较了接受传统他克莫司(CTAC)的患者与接受缓释他克莫司(ETAC)的患者的肾功能。
对海德堡心脏移植中心150例HTX患者的数据进行回顾性分析。所有患者在HTX后前2年内持续接受主要应用的钙调神经磷酸酶抑制剂,并根据中心惯例接受随访。
在HTX后前2年内,接受CSA的患者血清肌酐显著升高(P<0.0001),而接受TAC的患者血清肌酐变化无统计学意义(P=无统计学意义[ns])。McNemar检验发现,接受CSA的患者在HTX后上半年肾功能恶化的患者有显著聚集(P=0.0004)。在接受TAC的患者中,在HTX后前2年内未检测到肾功能恶化患者的显著聚集(所有P=ns)。接受CTAC与接受ETAC的患者的直接比较发现,在研究期间主要接受CTAC或ETAC治疗的患者之间,肾功能无显著差异(所有P=ns)。
与接受TAC作为基线免疫抑制治疗的患者相比,CSA与更明显的肾功能恶化相关,尤其是在HTX后的前6个月。