Stefan Mihaela S, Nathanson Brian H, Higgins Thomas L, Steingrub Jay S, Lagu Tara, Rothberg Michael B, Lindenauer Peter K
1Center for Quality of Care Research, Baystate Medical Center, Springfield, MA. 2Department of General Internal Medicine, Baystate Medical Center, Springfield, MA. 3Tufts Clinical and Translational Science Institute and Tufts University School of Medicine, Boston, MA. 4OptiStatim LLC, Longmeadow, MA. 5Division of Pulmonary and Critical Care Medicine, Baystate Medical Center, Springfield, MA. 6Center for Value-Based Care Research, Medicine Institute, Cleveland Clinic, Cleveland, OH.
Crit Care Med. 2015 Jul;43(7):1386-94. doi: 10.1097/CCM.0000000000000945.
To compare the characteristics and hospital outcomes of patients with an acute exacerbation of chronic obstructive pulmonary disease treated in the ICU with initial noninvasive ventilation or invasive mechanical ventilation.
Retrospective, multicenter cohort study of prospectively collected data. We used propensity matching to compare the outcomes of patients treated with noninvasive ventilation to those treated with invasive mechanical ventilation. We also assessed predictors for noninvasive ventilation failure.
Thirty-eight hospitals participating in the Acute Physiology and Chronic Health Evaluation database from 2008 through 2012.
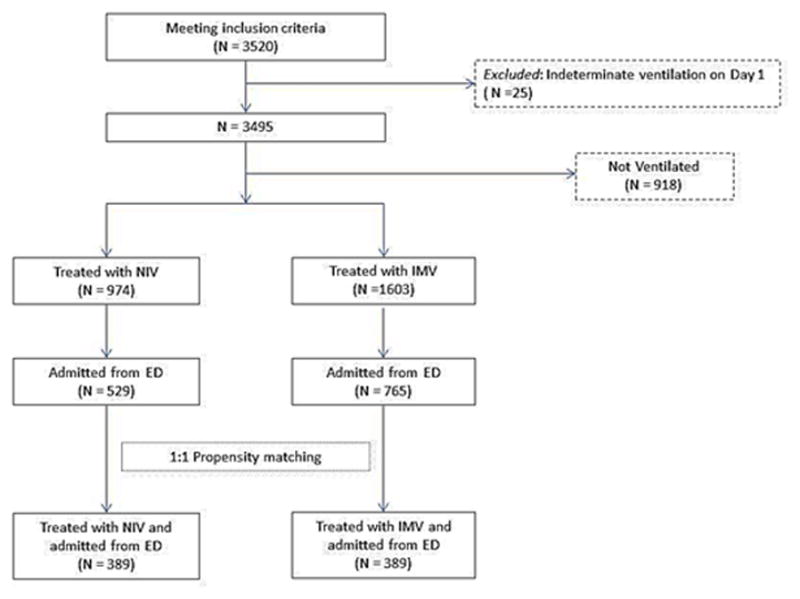
A total of 3,520 patients with a diagnosis of chronic obstructive pulmonary disease exacerbation including 27.7% who received noninvasive ventilation and 45.5% who received invasive mechanical ventilation.
None.
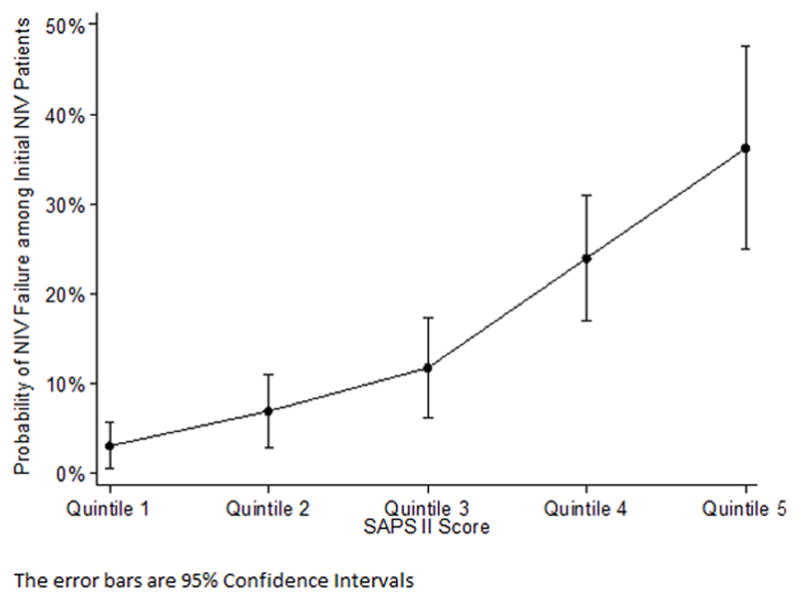
Noninvasive ventilation failure was recorded in 13.7% from patients ventilated noninvasively. Hospital mortality was 7.4% for patients treated with noninvasive ventilation; 16.1% for those treated with invasive mechanical ventilation; and 22.5% for those who failed noninvasive ventilation. In the propensity-matched analysis, patients initially treated with noninvasive ventilation had a 41% lower risk of death compared with those treated with invasive mechanical ventilation (relative risk, 0.59; 95% CI, 0.36-0.97). Factors that were independently associated with noninvasive ventilation failure were Simplified Acute Physiology Score II (relative risk = 1.04 per point increase; 95% CI, 1.03-1.04) and the presence of cancer (2.29; 95% CI, 0.96-5.45).
Among critically ill adults with chronic obstructive pulmonary disease exacerbation, the receipt of noninvasive ventilation was associated with a lower risk of in-hospital mortality compared with that of invasive mechanical ventilation; noninvasive ventilation failure was associated with the worst outcomes. These results support the use of noninvasive ventilation as a first-line therapy in appropriately selected critically ill patients with chronic obstructive pulmonary disease while also highlighting the risks associated with noninvasive ventilation failure and the need to be cautious in the face of severe disease.
比较在重症监护病房(ICU)接受初始无创通气或有创机械通气治疗的慢性阻塞性肺疾病急性加重患者的特征及住院结局。
对前瞻性收集的数据进行回顾性多中心队列研究。我们采用倾向匹配法比较接受无创通气治疗的患者与接受有创机械通气治疗的患者的结局。我们还评估了无创通气失败的预测因素。
2008年至2012年参与急性生理与慢性健康状况评估数据库的38家医院。
共有3520例诊断为慢性阻塞性肺疾病急性加重的患者,其中27.7%接受无创通气,45.5%接受有创机械通气。
无。
无创通气患者中13.7%记录有无创通气失败。接受无创通气治疗的患者医院死亡率为7.4%;接受有创机械通气治疗的患者为16.1%;无创通气失败的患者为22.5%。在倾向匹配分析中,初始接受无创通气治疗的患者死亡风险比接受有创机械通气治疗的患者低41%(相对风险,0.59;95%可信区间,0.36 - 0.97)。与无创通气失败独立相关的因素为简化急性生理学评分II(每增加1分相对风险 = 1.04;95%可信区间,1.03 - 1.04)和癌症的存在(2.29;95%可信区间,0.96 - 5.45)。
在患有慢性阻塞性肺疾病急性加重的重症成年患者中,与有创机械通气相比,接受无创通气与较低的院内死亡风险相关;无创通气失败与最差的结局相关。这些结果支持在适当选择的患有慢性阻塞性肺疾病的重症患者中使用无创通气作为一线治疗方法,同时也强调了无创通气失败相关的风险以及面对严重疾病时需谨慎的必要性。