Interiano Rodrigo B, McCarville M Beth, Wu Jianrong, Davidoff Andrew M, Sandoval John, Navid Fariba
Department of Surgery, St. Jude Children's Research Hospital, Memphis, TN 38105, USA; Department of Surgery, College of Medicine, University of Tennessee Health Science Center, Memphis, TN 38163, USA.
Department of Radiological Sciences, St. Jude Children's Research Hospital, Memphis, TN 38105, USA; Department of Radiology, College of Medicine, University of Tennessee Health Science Center, Memphis, TN 38163, USA.
J Pediatr Surg. 2015 Sep;50(9):1484-9. doi: 10.1016/j.jpedsurg.2015.01.005. Epub 2015 Jan 16.
Antiangiogenic agents show significant antitumor activity against various tumor types. In a study evaluating the combination of sorafenib, bevacizumab, and low-dose cyclophosphamide in children with solid tumors, an unexpectedly high incidence of pneumothorax was observed. We evaluated patient characteristics and risk factors for the development of pneumothorax in patients receiving this therapy.
Demographics, clinical course, and radiographic data of 44 patients treated with sorafenib, bevacizumab and cyclophosphamide were reviewed. Risk factors associated with the development of pneumothorax were analyzed.
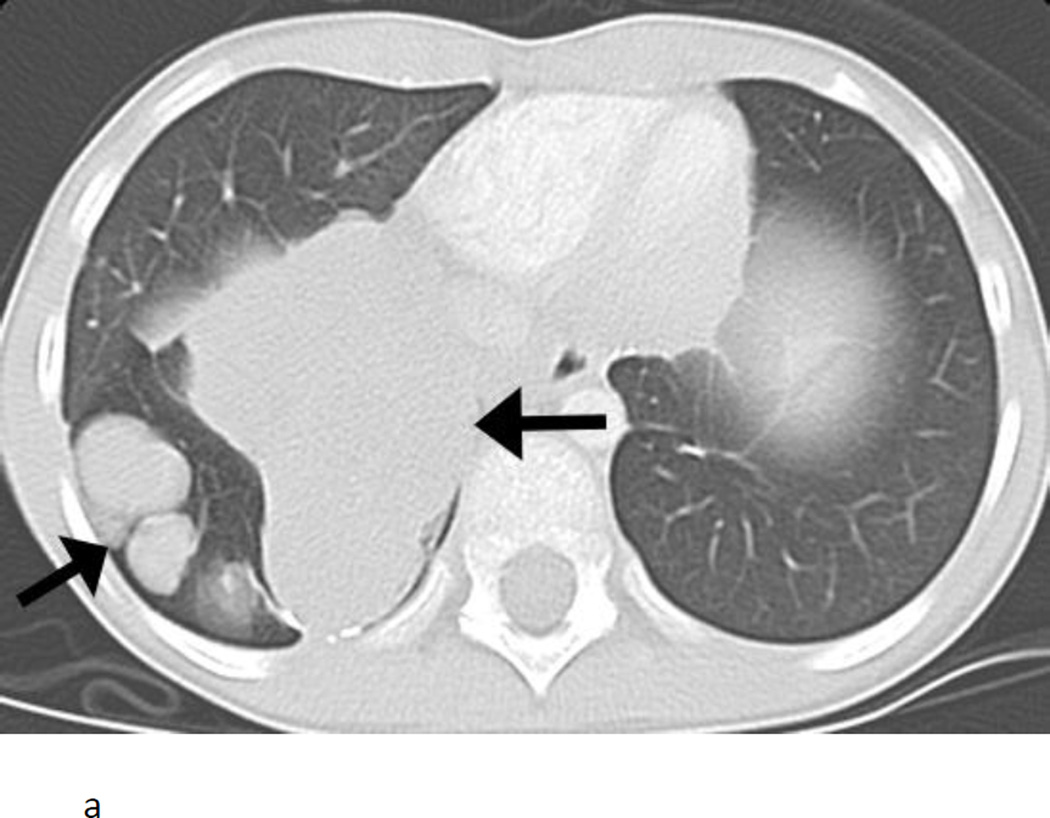
Pneumothorax likely related to study therapy developed in 11 of 44 (25%) patients of whom 33 had pulmonary abnormalities. Median age of patients was 14.7 years (range, 1.08-24.5). Histologies associated with pneumothorax included rhabdoid tumor, synovial sarcoma, osteosarcoma, Ewing sarcoma, Wilms tumor, and renal cell carcinoma. Cavitation of pulmonary nodules in response to therapy was associated with pneumothorax development (P<0.001). Median time from start of therapy to development of pneumothorax was 5.7 weeks (range, 2.4-31).
The development of cavitary pulmonary nodules in response to therapy is a risk factor for pneumothorax. As pneumothorax is a potentially life-threatening complication of antiangiogenic therapy in children with solid tumors, its risk needs to be evaluated when considering this therapy.
抗血管生成药物对多种肿瘤类型显示出显著的抗肿瘤活性。在一项评估索拉非尼、贝伐单抗和低剂量环磷酰胺联合治疗实体瘤患儿的研究中,观察到气胸发生率意外地高。我们评估了接受该治疗的患者发生气胸的特征和危险因素。
回顾了44例接受索拉非尼、贝伐单抗和环磷酰胺治疗的患者的人口统计学、临床病程和影像学数据。分析了与气胸发生相关的危险因素。
44例患者中有11例(25%)发生了可能与研究治疗相关的气胸,其中33例有肺部异常。患者的中位年龄为14.7岁(范围1.08 - 24.5岁)。与气胸相关的组织学类型包括横纹肌样瘤、滑膜肉瘤、骨肉瘤、尤因肉瘤、肾母细胞瘤和肾细胞癌。治疗后肺结节空洞形成与气胸发生相关(P<0.001)。从治疗开始到发生气胸的中位时间为5.7周(范围2.4 - 31周)。
治疗后肺空洞性结节的形成是气胸的一个危险因素。由于气胸是实体瘤患儿抗血管生成治疗的一种潜在危及生命的并发症,在考虑这种治疗时需要评估其风险。