Klop C, Welsing P M J, Elders P J M, Overbeek J A, Souverein P C, Burden A M, van Onzenoort H A W, Leufkens H G M, Bijlsma J W J, de Vries F
Utrecht Institute for Pharmaceutical Sciences, Division of Pharmacoepidemiology and Clinical Pharmacology, Utrecht University, Utrecht, Netherlands.
Department of Rheumatology and Clinical Immunology, University Medical Center, Utrecht, Netherlands.
Osteoporos Int. 2015 Jun;26(6):1831-40. doi: 10.1007/s00198-015-3084-3. Epub 2015 Mar 31.
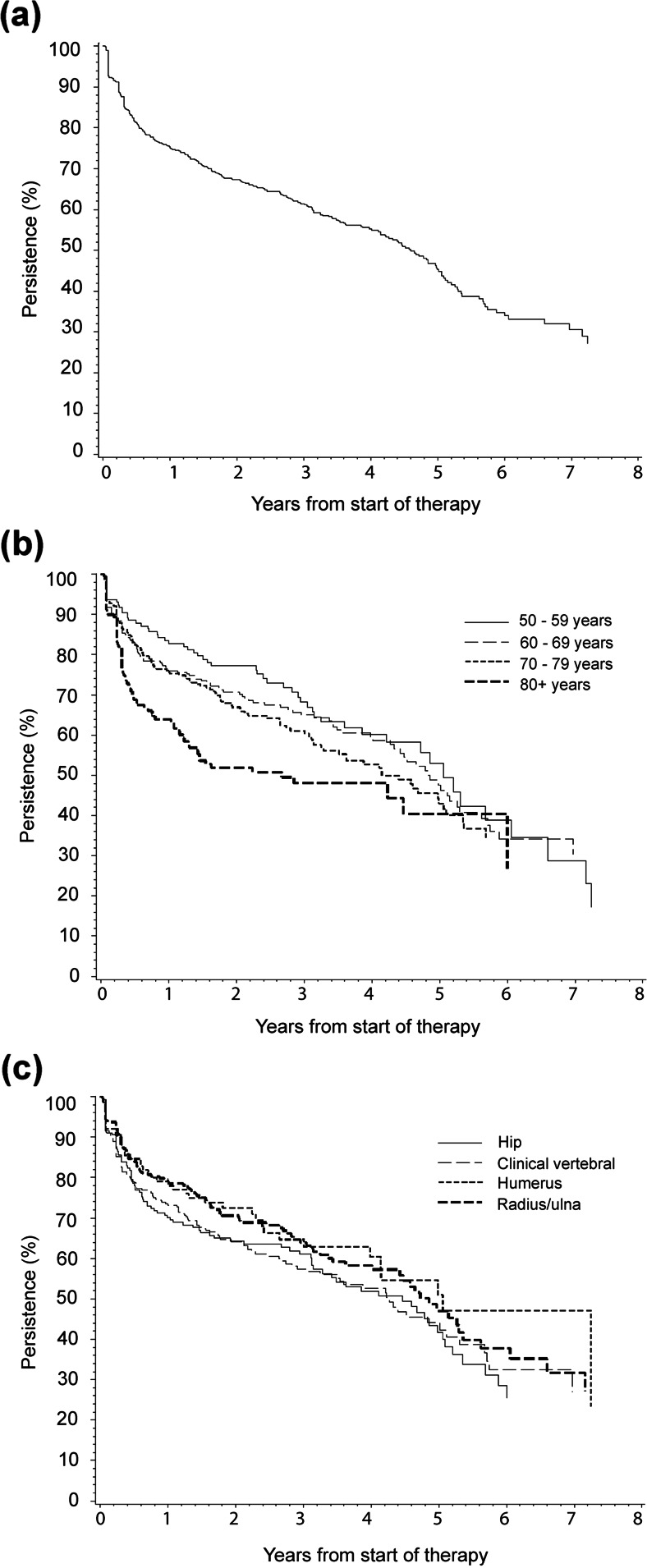
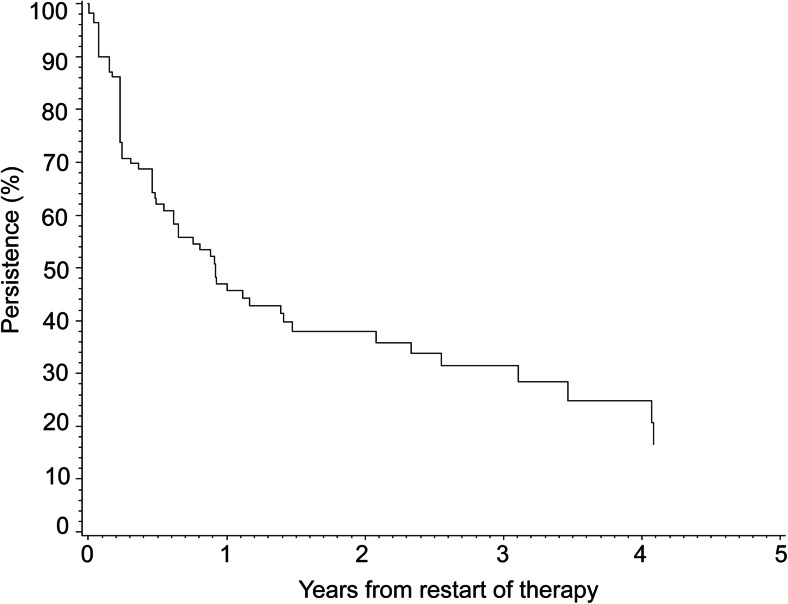
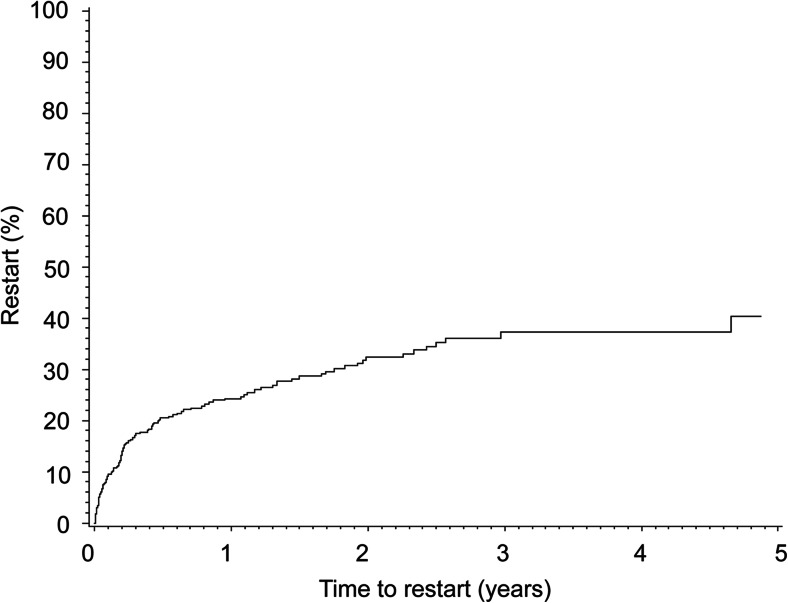
Long-term persistence with anti-osteoporosis drugs and determinants for discontinuation among fracture patients were examined. Persistence was 75.0 and 45.3 % after 1 and 5 years, respectively. Those aged ≥80 years were at increased risk of early discontinuation. Within 1 year after discontinuation, 24.3 % restarted therapy, yet 47.0 % persisted for 1 year.
The risk of osteoporotic fracture can effectively be reduced with use of anti-osteoporosis drugs. However, little is known about persistence with these drugs after fracture where subsequent fracture risk is high. The aims were to determine long-term persistence with anti-osteoporosis drugs among fracture patients, including its determinants, and to describe restart and subsequent persistence.
A cohort study was conducted within the Dutch PHARMO Database Network. Patients aged ≥50 years (n = 961) who received anti-osteoporosis drugs within 1 year after fracture, but not in the preceding year, were included (2002-2011). Persistence (defined as the proportion on treatment) and the proportion restarting after discontinuation were estimated using Kaplan-Meier analyses. Time-dependent Cox regression was used to identify determinants of non-persistence including age, sex, initial dosage regime, fracture type, comorbidities, and drug use.
Persistence with anti-osteoporosis drugs was 75.0 % (95 % confidence interval (CI) 72.0-77.7) and 45.3 % (95 % CI 40.4-50.0) after 1 and 5 years, respectively. A significant determinant of non-persistence was age ≥80 years (reference 50-59 years: adjusted hazard ratio [adj. HR] 1.65; 95 % CI 1.15-2.38). This effect was not constant over time (≤360 days following initiation: adj. HR 2.07; 95 % CI 1.27-3.37; >360 days: adj. HR 1.08; 95 % CI 0.62-1.88). Within 1 year after discontinuation, 24.3 % (95 % CI 20.1-29.2) restarted therapy, yet 47.0 % persisted for 1 year.
This study identified suboptimal persistence with anti-osteoporosis drugs among fracture patients. Major target groups for measures aimed to improve persistence may be those aged >80 years and those restarting therapy.
研究了骨折患者抗骨质疏松药物的长期持续性及停药的决定因素。1年和5年后的持续性分别为75.0%和45.3%。年龄≥80岁的患者早期停药风险增加。停药后1年内,24.3%的患者重新开始治疗,但47.0%的患者持续用药1年。
使用抗骨质疏松药物可有效降低骨质疏松性骨折的风险。然而,对于骨折后后续骨折风险较高时这些药物的持续性知之甚少。目的是确定骨折患者抗骨质疏松药物的长期持续性,包括其决定因素,并描述重新开始用药及后续的持续性情况。
在荷兰PHARMO数据库网络内进行了一项队列研究。纳入了年龄≥50岁(n = 961)、在骨折后1年内但非前一年接受抗骨质疏松药物治疗的患者(2002 - 2011年)。使用Kaplan - Meier分析估计持续性(定义为治疗患者的比例)及停药后重新开始治疗的比例。采用时间依赖性Cox回归确定非持续性的决定因素,包括年龄、性别、初始剂量方案、骨折类型、合并症和药物使用情况。
抗骨质疏松药物治疗1年和5年后的持续性分别为75.0%(95%置信区间[CI] 72.0 - 77.7)和45.3%(95% CI 40.4 - 50.0)。非持续性的一个显著决定因素是年龄≥80岁(参考年龄50 - 59岁:调整后风险比[adj. HR] 1.65;95% CI 1.15 - 2.38)。这种影响随时间并非恒定(开始治疗后≤360天:adj. HR 2.07;95% CI 1.27 - 3.37;>360天:adj. HR 1.08;95% CI 0.62 - 1.88)。停药后1年内,24.3%(95% CI 20.1 - 29.2)的患者重新开始治疗,但47.0%的患者持续用药1年。
本研究发现骨折患者抗骨质疏松药物的持续性欠佳。旨在提高持续性的措施的主要目标群体可能是年龄>80岁的患者及重新开始治疗的患者。