Meshaal Marwa Sayed, Kassem Hussein Heshmat, Samir Ahmad, Zakaria Ayman, Baghdady Yasser, Rizk Hussein Hassan
Department of Cardiovascular Medicine, Cairo University, Cairo, Egypt.
Department of Radiology, Cairo University, Cairo, Egypt.
PLoS One. 2015 Mar 30;10(3):e0118616. doi: 10.1371/journal.pone.0118616. eCollection 2015.
Infective endocarditis (IE) is commonly complicated by cerebral embolization and hemorrhage secondary to intracranial mycotic aneurysms (ICMAs). These complications are associated with poor outcome and may require diagnostic and therapeutic plans to be modified. However, routine screening by brain CT and CT angiography (CTA) is not standard practice. We aimed to study the impact of routine cerebral CTA on treatment decisions for patients with IE.
From July 2007 to December 2012, we prospectively recruited 81 consecutive patients with definite left-sided IE according to modified Duke's criteria. All patients had routine brain CTA conducted within one week of admission. All patients with ICMA underwent four-vessel conventional angiography. Invasive treatment was performed for ruptured aneurysms, aneurysms ≥ 5 mm, and persistent aneurysms despite appropriate therapy. Surgical clipping was performed for leaking aneurysms if not amenable to intervention.
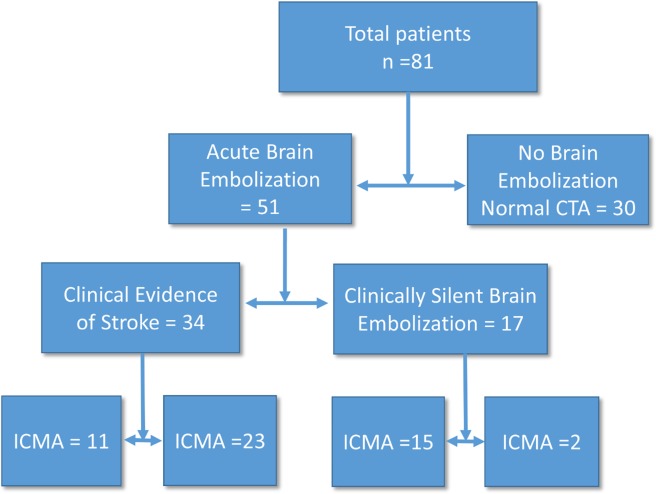
The mean age was 30.43 ± 8.8 years and 60.5% were males. Staph aureus was the most common organism (32.3%). Among the patients, 37% had underlying rheumatic heart disease, 26% had prosthetic valves, 23.5% developed IE on top of a structurally normal heart and 8.6% had underlying congenital heart disease. Brain CT/CTA revealed that 51 patients had evidence of cerebral embolization, of them 17 were clinically silent. Twenty-six patients (32%) had ICMA, of whom 15 were clinically silent. Among the patients with ICMAs, 11 underwent endovascular treatment and 2 underwent neurovascular surgery. The brain CTA findings prompted different treatment choices in 21 patients (25.6%). The choices were aneurysm treatment before cardiac surgery rather than at follow-up, valve replacement by biological valve instead of mechanical valve, and withholding anticoagulation in patients with prosthetic valve endocarditis for fear of aneurysm rupture.
Routine brain CT/CTA resulted in changes in the treatment plan in a significant proportion of patients with IE, even those without clinically evident neurological disease. Routine brain CT/CTA may be indicated in all hospitalized patients with IE.
感染性心内膜炎(IE)常因颅内真菌性动脉瘤(ICMA)继发脑栓塞和出血而并发。这些并发症与不良预后相关,可能需要修改诊断和治疗方案。然而,通过脑部CT和CT血管造影(CTA)进行常规筛查并非标准做法。我们旨在研究常规脑部CTA对IE患者治疗决策的影响。
2007年7月至2012年12月,我们根据改良的杜克标准前瞻性招募了81例连续的确诊左侧IE患者。所有患者在入院后一周内进行了常规脑部CTA检查。所有ICMA患者均接受了四血管常规血管造影。对破裂的动脉瘤、直径≥5mm的动脉瘤以及经适当治疗后仍持续存在的动脉瘤进行了侵入性治疗。对于渗漏性动脉瘤,如果不适合介入治疗,则进行手术夹闭。
平均年龄为30.43±8.8岁,男性占60.5%。金黄色葡萄球菌是最常见的病原体(32.3%)。在患者中,37%有潜在的风湿性心脏病,26%有人工瓣膜,23.5%在结构正常的心脏基础上发生IE,8.6%有潜在的先天性心脏病。脑部CT/CTA显示,51例患者有脑栓塞证据,其中17例临床无症状。26例患者(32%)有ICMA,其中15例临床无症状。在ICMA患者中,11例接受了血管内治疗,2例接受了神经血管手术。脑部CTA检查结果促使21例患者(25.6%)做出了不同的治疗选择。这些选择包括在心脏手术前而非随访时进行动脉瘤治疗、用生物瓣膜而非机械瓣膜进行瓣膜置换,以及因担心动脉瘤破裂而在人工瓣膜心内膜炎患者中停用抗凝治疗。
常规脑部CT/CTA使相当一部分IE患者的治疗方案发生了改变,即使是那些没有临床明显神经疾病的患者。所有住院的IE患者可能都需要进行常规脑部CT/CTA检查。