Pathik Parikh, Ravindra Surude, Ajay Choksey, Prasad Bhate, Jatin Patel, Prabha Sawant
Department of Gastroenterology, Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai, India.
Ann Gastroenterol. 2015 Apr-Jun;28(2):281-286.
The aim of the study was to determine the efficacy of Fibroscan versus noninvasive markers, i.e. nonalcoholic fatty liver disease (NAFLD) fibrosis score (NFS); Aspartate-aminotransferase (AST)/platelet ratio (APRI); and AST/Alanine-aminotransferase (AAR) as a screening tool in NAFLD patients with high risk of liver fibrosis.
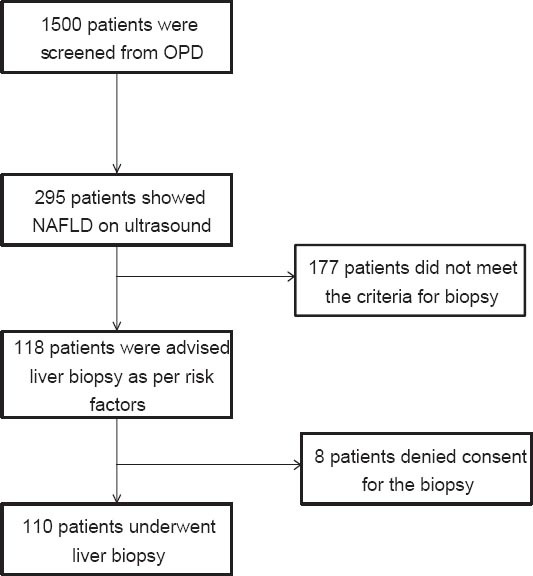
This is a single-center study carried out in patients attending the outpatient department for dyspepsia and diagnosed with fatty liver on ultrasound. Liver biopsy was advised in diabetics, metabolic syndrome, body mass index >30 kg/m, raised transaminases and hypothyroidism. Fibroscan, APRI, AAR and NFS were calculated. Area under the curve (AUROC), negative (NPV) and positive predictive values (PPV) were calculated for each diagnostic test.
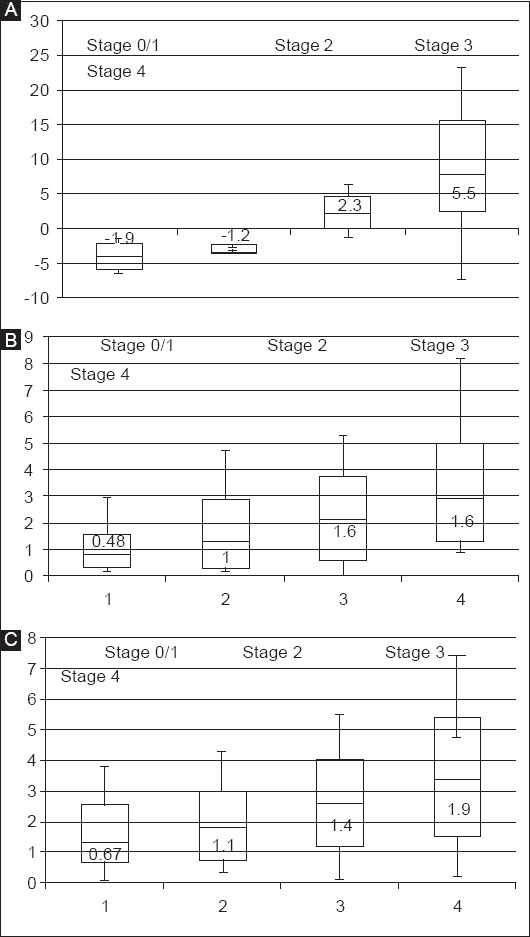
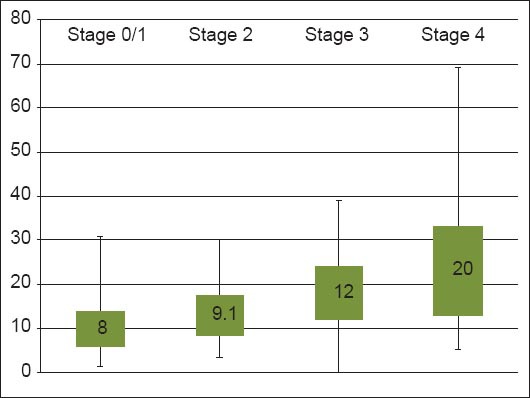
Of the 1500 patients screened, 110 with the above-described risk factors underwent liver biopsy (stage 3/4 fibrosis = 38). Diabetes predicted severe fibrosis (stage 3/4). Sensitivity, specificity, PPV, NPV and AUROC for Fibroscan at value 12 kPa were 0.9, 0.8, 0.70, 0.93 and 0.91 respectively for predicting stage 3/4 fibrosis. With increase in severity of liver fibrosis there was stepwise increase in Fibroscan values (P=0.000038, Kruskal-Wallis test). Sensitivity, specificity, PPV and NPV for AAR and NFS at cutoff of 1.5 and 0.676 were 0.8, 1.0, 1.0 and 0.92 and 0.8, 1.0, 1.0 and 0.92 respectively.
Fibroscan, NFS and AAR are simple noninvasive markers of fibrosis that can be utilized as screening tools in patients with high risk for fibrosis to determine the need for biopsy. The cutoff of Fibroscan for stage 3/4 fibrosis was 12 kPa.
本研究的目的是确定Fibroscan与非侵入性标志物,即非酒精性脂肪性肝病(NAFLD)纤维化评分(NFS)、天冬氨酸转氨酶(AST)/血小板比值(APRI)以及AST/丙氨酸转氨酶比值(AAR)作为肝纤维化高风险NAFLD患者筛查工具的有效性。
这是一项单中心研究,研究对象为因消化不良到门诊就诊且经超声诊断为脂肪肝的患者。对于糖尿病患者、代谢综合征患者、体重指数>30kg/m²、转氨酶升高以及甲状腺功能减退患者,建议进行肝活检。计算Fibroscan、APRI、AAR和NFS。计算每种诊断试验的曲线下面积(AUROC)、阴性预测值(NPV)和阳性预测值(PPV)。
在筛查的1500例患者中,110例有上述风险因素的患者接受了肝活检(3/4期纤维化 = 38例)。糖尿病可预测严重纤维化(3/4期)。Fibroscan值为12kPa时,预测3/4期纤维化的敏感性、特异性、PPV、NPV和AUROC分别为0.9、0.8、0.70、0.93和0.91。随着肝纤维化严重程度增加,Fibroscan值呈逐步升高趋势(P = 0.000038,Kruskal-Wallis检验)。AAR和NFS在临界值为1.5和0.676时的敏感性、特异性、PPV和NPV分别为0.8、1.0、1.0和0.92以及0.8、1.0、1.0和0.92。
Fibroscan、NFS和AAR是简单的非侵入性纤维化标志物,可作为纤维化高风险患者的筛查工具,以确定是否需要进行活检。Fibroscan诊断3/4期纤维化的临界值为12kPa。