Department of Surgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Department of Surgery, Eulji General Hospital, Eulji University College of Medicine, Seoul, Korea.
J Breast Cancer. 2015 Mar;18(1):29-35. doi: 10.4048/jbc.2015.18.1.29. Epub 2015 Mar 27.
To investigate treatment options for local control of metastasis in the brain, we compared focal brain treatment (FBT) with or without whole brain radiotherapy (WBRT) vs. WBRT alone, for breast cancer patients with tumor relapse in the brain. We also evaluated treatment outcomes according to the subtypes.
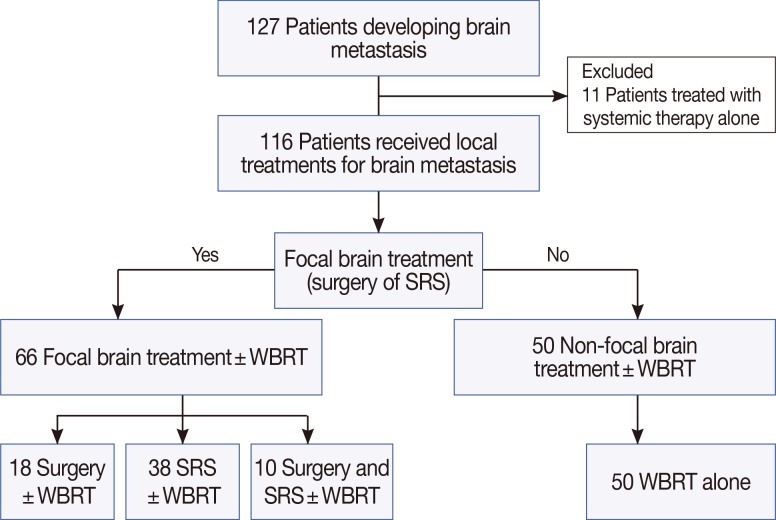
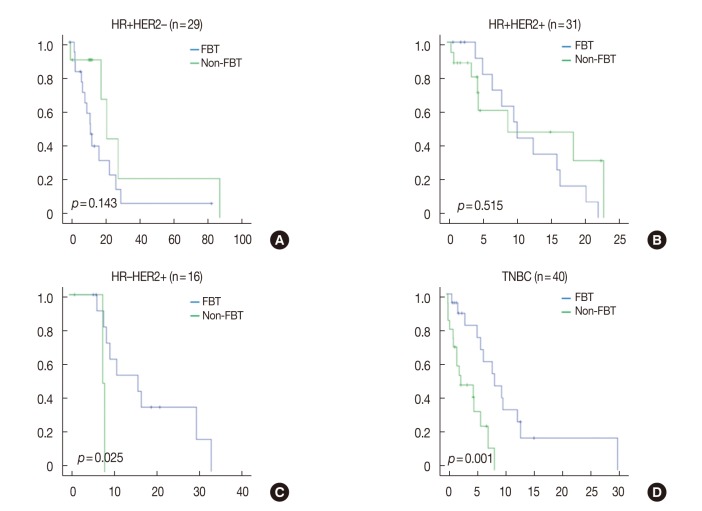
We conducted a retrospective review of breast cancer patients with brain metastasis after primary surgery. All patients received at least one local treatment for brain metastasis. Surgery or stereotactic radiosurgery was categorized as FBT. Patients were divided into two groups: the FBT group received FBT±WBRT, whereas the non-FBT group received WBRT alone. Subtypes were defined as follows: hormone receptor (HR)-positive/human epidermal growth factor receptor 2 (HER2)-negative, HR-positive/HER2-positive, HR-negative/HER2-positive, and triple-negative (TN). We examined the overall survival after brain metastasis (OSBM), brain metastasis-specific survival (BMSS), and brain metastasis-specific progression-free survival (BMPFS).
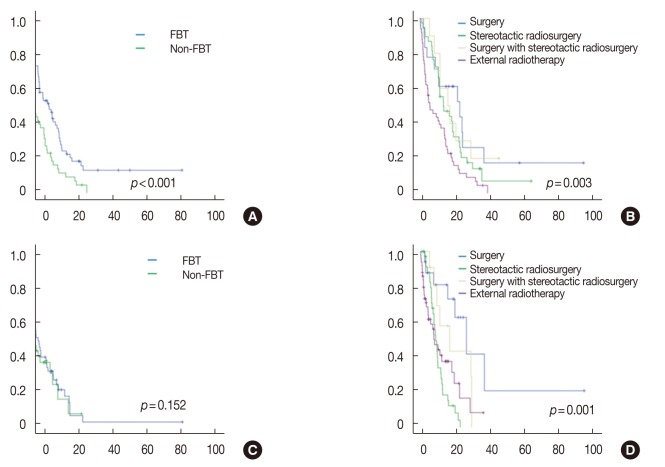
A total of 116 patients were identified. After a median follow-up of 50.9 months, the median OSBM was 11.5 months (95% confidence interval, 9.0-14.1 months). The FBT group showed significantly superior OSBM and BMSS. However, FBT was not an independent prognostic factor for OSBM and BMSS on multivariate analyses. In contrast, multivariate analyses showed that patients who underwent surgery had improved BMPFS, indicating local control of metastasis in the brain. FBT resulted in better BMPFS in patients with HR-negative/HER2-positive cancer or the TN subtype.
We found that patients who underwent surgery experienced improved local control of brain metastasis, regardless of its extent. Furthermore, FBT showed positive results and could be considered for better local control of brain metastasis in patients with aggressive subtypes such as HER2-positive and TN.
为了研究局部控制脑转移的治疗选择,我们比较了局部脑治疗(FBT)联合或不联合全脑放疗(WBRT)与单纯 WBRT 治疗乳腺癌脑转移患者的疗效。我们还根据亚型评估了治疗结果。
我们对原发性手术后脑转移的乳腺癌患者进行了回顾性研究。所有患者均接受了至少一次脑转移局部治疗。手术或立体定向放射外科被归类为 FBT。患者分为两组:FBT 组接受 FBT±WBRT,而非 FBT 组仅接受 WBRT。亚型定义如下:激素受体(HR)阳性/人表皮生长因子受体 2(HER2)阴性、HR 阳性/HER2 阳性、HR 阴性/HER2 阳性和三阴性(TN)。我们检查了脑转移后总生存期(OSBM)、脑转移特异性生存期(BMSS)和脑转移特异性无进展生存期(BMPFS)。
共纳入 116 例患者。中位随访 50.9 个月后,中位 OSBM 为 11.5 个月(95%置信区间,9.0-14.1 个月)。FBT 组的 OSBM 和 BMSS 显著提高。然而,多因素分析显示,FBT 不是 OSBM 和 BMSS 的独立预后因素。相反,多因素分析表明,接受手术的患者 BMPFS 得到改善,表明脑转移的局部控制得到改善。FBT 使 HR 阴性/HER2 阳性或 TN 型患者的 BMPFS 更好。
我们发现,无论脑转移的范围如何,接受手术的患者都能更好地控制脑转移的局部进展。此外,FBT 显示出积极的结果,对于 HER2 阳性和 TN 等侵袭性亚型的患者,可考虑更好地控制脑转移的局部进展。