McKay Ailsa J, Patel Raju K K, Majeed Azeem
Department of Primary Care and Public Health, Imperial College London, London, United Kingdom.
London North West Healthcare NHS Trust, London, United Kingdom.
PLoS One. 2015 Apr 9;10(4):e0122610. doi: 10.1371/journal.pone.0122610. eCollection 2015.
Tobacco control needs in India are large and complex. Evaluation of outcomes to date has been limited.
To review the extent of tobacco control measures, and the outcomes of associated trialled interventions, in India.
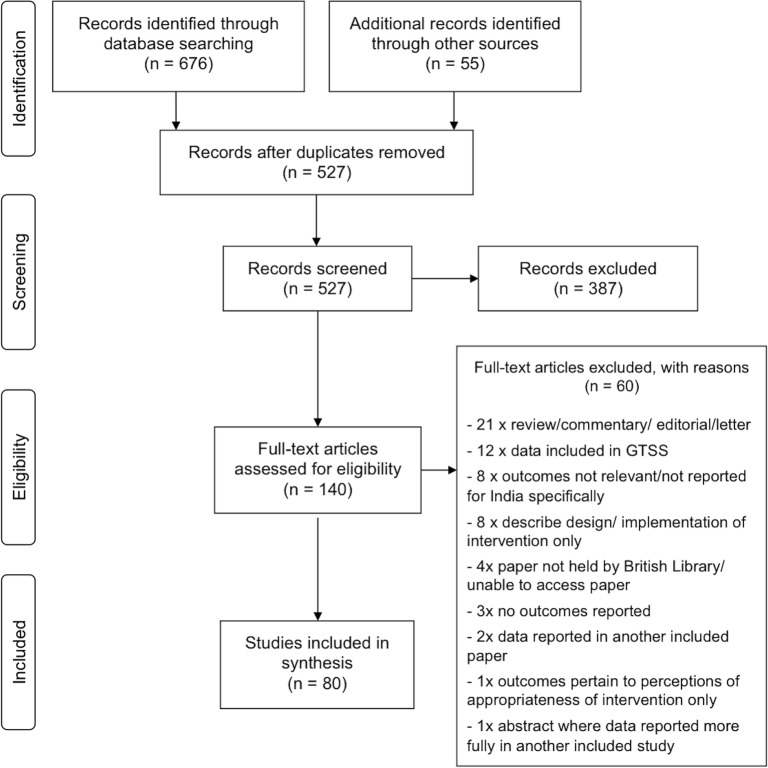
Information was identified via database searches, journal hand-searches, reference and citation searching, and contact with experts. Studies of any population resident in India were included. Studies where outcomes were not yet available, not directly related to tobacco use, or not specific to India, were excluded. Pre-tested proformas were used for data extraction and quality assessment. Studies with reliability concerns were excluded from some aspects of analysis. The Framework Convention on Tobacco Control (FCTC) was use as a framework for synthesis. Heterogeneity limited meta-analysis options. Synthesis was therefore predominantly narrative.
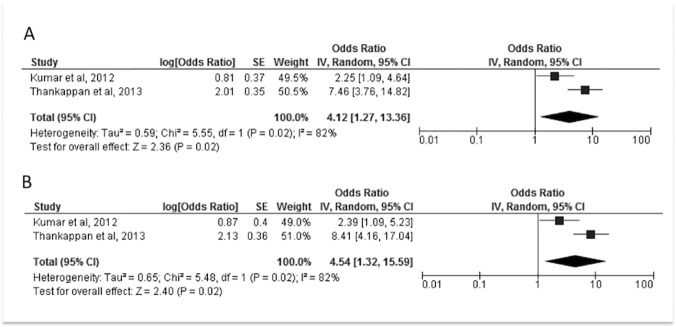
Additional to the Global Tobacco Surveillance System data, 80 studies were identified, 45 without reliability concerns. Most related to education (FCTC Article 12) and tobacco-use cessation (Article 14). They indicated widespread understanding of tobacco-related harm, but less knowledge about specific consequences of use. Healthcare professionals reported low confidence in cessation assistance, in keeping with low levels of training. Training for schoolteachers also appeared suboptimal. Educational and cessation assistance interventions demonstrated positive impact on tobacco use. Studies relating to smoke-free policies (Article 8), tobacco advertisements and availability (Articles 13 and 16) indicated increasingly widespread smoke-free policies, but persistence of high levels of SHS exposure, tobacco promotions and availability-including to minors. Data relating to taxation/pricing and packaging (Articles 6 and 11) were limited. We did not identify any studies of product regulation, alternative employment strategies, or illicit trade (Articles 9, 10, 15 and 17).
Tobacco-use outcomes could be improved by school/community-based and adult education interventions, and cessation assistance, facilitated by training for health professionals and schoolteachers. Additional tobacco control measures should be assessed.
印度的烟草控制需求巨大且复杂。迄今为止,对相关成果的评估有限。
回顾印度烟草控制措施的实施程度以及相关试验性干预措施的成果。
通过数据库检索、期刊手工检索、参考文献和引文检索以及与专家联系来获取信息。纳入对印度任何居民群体的研究。排除那些尚未得出结果、与烟草使用无直接关联或并非针对印度的研究。使用预先测试的表格进行数据提取和质量评估。对可靠性存疑的研究在某些分析方面被排除。以《烟草控制框架公约》(FCTC)作为综合框架。异质性限制了荟萃分析的选择。因此,综合主要采用叙述性方式。
除全球烟草监测系统的数据外,共识别出80项研究,其中45项不存在可靠性问题。大多数研究与教育(FCTC第12条)和戒烟(第14条)相关。这些研究表明人们对烟草相关危害有广泛的认识,但对使用烟草的具体后果了解较少。医疗保健专业人员报告称在戒烟援助方面信心不足,这与培训水平较低相符。对学校教师的培训似乎也不尽人意。教育和戒烟援助干预措施对烟草使用产生了积极影响。与无烟政策(第8条)、烟草广告和可得性(第13条和第16条)相关的研究表明,无烟政策日益普及,但二手烟暴露、烟草促销以及可得性(包括向未成年人提供烟草)的水平仍然居高不下。与税收/定价和包装(第6条和第11条)相关的数据有限。我们未识别出任何关于产品监管、替代就业策略或非法贸易(第9条、第10条、第15条和第17条)的研究。
通过以学校/社区为基础的教育干预、成人教育干预以及戒烟援助,同时辅以对医疗保健专业人员和学校教师培训,烟草使用情况有望得到改善。应评估更多烟草控制措施。