Maduna Patrick H, Dolan Matt, Kondlo Lwando, Mabuza Honey, Dlamini Judith N, Polis Mike, Mnisi Thabo, Orsega Susan, Maja Patrick, Ledwaba Lotty, Molefe Thuthukile, Sangweni Phumelele, Malan Lisette, Matchaba Gugu, Khabo Paul, Grandits Greg, Neaton James D
South Africa Military Health Services, South African National Defence Forces, Pretoria, South Africa.
The Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., Bethesda, Maryland, United States of America.
PLoS One. 2015 Apr 9;10(4):e0121843. doi: 10.1371/journal.pone.0121843. eCollection 2015.
Short-term morbidity and mortality rates for HIV positive soldiers in the South African National Defence Force (SANDF) would inform decisions about deployment and HIV disease management. Risks were determined according to the latest CD4+ cell count and use of antiretroviral therapy (ART) for HIV positive individuals in the SANDF and their dependents.
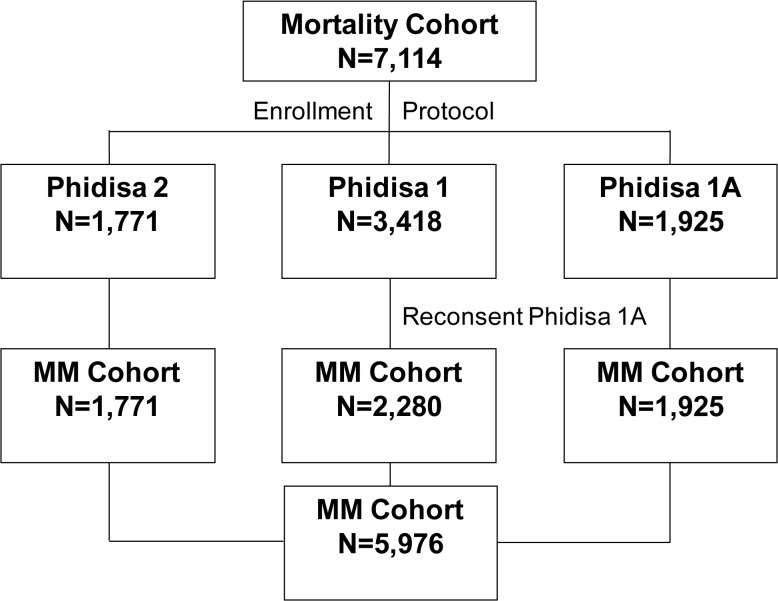
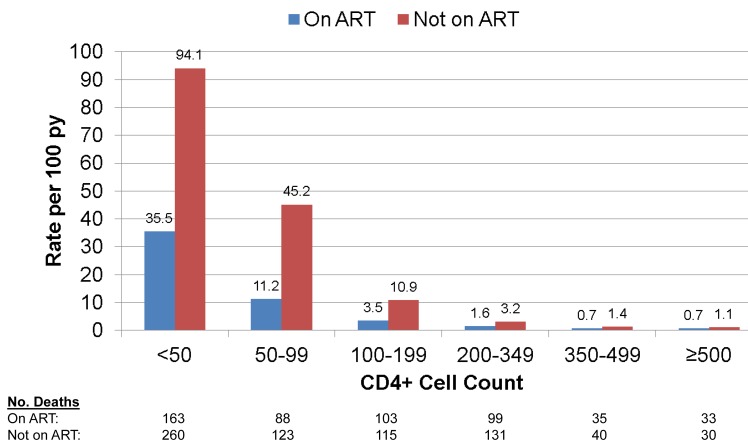
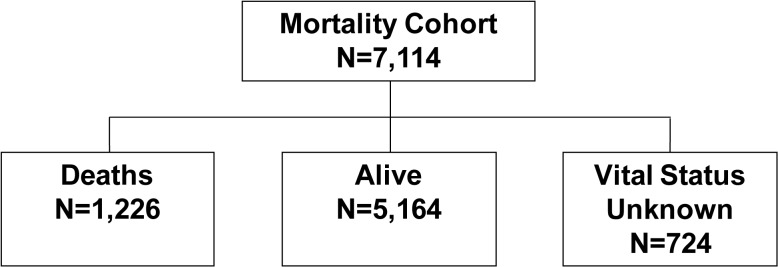
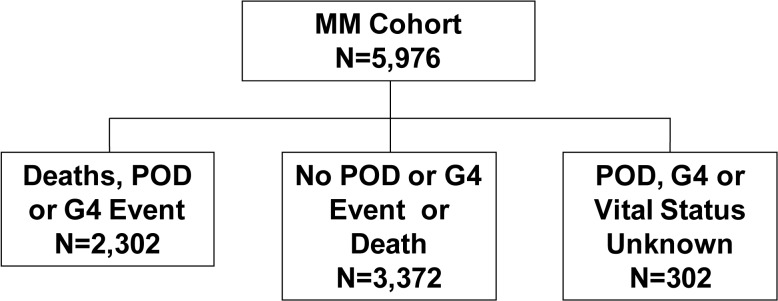
A total of 7,114 participants were enrolled and followed for mortality over a median of 4.7 years (IQR: 1.9, 7.1 years). For a planned subset (5,976), progression of disease (POD) and grade 4, potentially life-threatening events were also ascertained. CD4+ count and viral load were measured every 3 to 6 months. Poisson regression was used to compare event rates by latest CD4+ count (<50, 50-99, 100-199, 200-349, 350-499, 500+) with a focus on upper three strata, and to estimate relative risks (RRs) (ART/no ART). Median entry CD4+ was 207 cells/mm3. During follow-up over 70% were prescribed ART. Over follow-up 1,226 participants died; rates ranged from 57.6 (< 50 cells) to 0.8 (500+ cells) per 100 person years (py). Compared to those with latest CD4+ 200-349 (2.2/100 py), death rates were significantly lower (p<0.001), as expected, for those with 350-499 (0.9/100 py) and with 500+ cells (0.8/100 py). The composite outcome of death, POD or grade 4 events occurred in 2,302 participants (4,045 events); rates were similar in higher CD4+ count strata (9.4 for 350-499 and 7.9 for 500+ cells) and lower than those with counts 200-349 cells (13.5) (p<0.001). For those with latest CD4+ 350+ cells, 63% of the composite outcomes (680 of 1,074) were grade 4 events.
Rates of morbidity and mortality are lowest among those with CD4+ count of 350 or higher and rates do not differ for those with counts of 350-499 versus 500+ cells. Grade 4 events are the predominant morbidity for participants with CD4+ counts of 350+ cells.
南非国防军(SANDF)中HIV阳性士兵的短期发病率和死亡率可为部署决策及HIV疾病管理提供依据。根据南非国防军及其家属中HIV阳性个体的最新CD4+细胞计数和抗逆转录病毒疗法(ART)的使用情况来确定风险。
共纳入7114名参与者,中位随访4.7年(四分位间距:1.9,7.1年)以观察死亡率。对于一个计划中的亚组(5976人),还确定了疾病进展(POD)和4级潜在危及生命的事件。每3至6个月测量一次CD4+计数和病毒载量。使用泊松回归比较最新CD4+计数(<50、50 - 99、100 - 199、200 - 349、350 - 499、500+)的事件发生率,重点关注最高的三个分层,并估计相对风险(RRs)(接受ART/未接受ART)。入组时CD4+的中位数为207个细胞/mm³。随访期间超过70%的参与者接受了ART治疗。随访期间1226名参与者死亡;每100人年(py)的死亡率范围从57.6(<五十个细胞)到0.8(500+个细胞)。与最新CD4+为200 - 349(2.2/100 py)的参与者相比,正如预期的那样,CD4+为350 - 499(0.9/100 py)和500+个细胞(0.8/100 py)的参与者死亡率显著更低(p<0.001)。2302名参与者(4045起事件)发生了死亡、POD或4级事件的综合结局;较高CD4+计数分层中的发生率相似(350 - 499为9.4,500+个细胞为7.9),且低于CD4+计数为200 - 349个细胞的分层(13.5)(p<0.001)。对于最新CD4+为350+个细胞的参与者,综合结局的63%(1074例中的680例)为4级事件。
CD4+计数为350或更高的人群中发病率和死亡率最低,CD4+计数为350 - 499与500+个细胞的人群发病率和死亡率无差异。4级事件是CD4+计数为350+个细胞的参与者的主要发病情况。