Bryant Richard J, Sjoberg Daniel D, Vickers Andrew J, Robinson Mary C, Kumar Rajeev, Marsden Luke, Davis Michael, Scardino Peter T, Donovan Jenny, Neal David E, Lilja Hans, Hamdy Freddie C
Nuffield Department of Surgical Sciences, University of Oxford, UK (RJB, RK, LM, HL, FCH); Department of Epidemiology & Biostatistics, Memorial Sloan Kettering Cancer Center, New York, NY (DDS, AJV); Department of Cellular Pathology, Royal Victoria Infirmary, Newcastle upon Tyne, UK (MCR); School of Social and Community Medicine, University of Bristol, UK (MD); Department of Surgery, Urology Service, Memorial Sloan Kettering Cancer Center (PTS, HL); Department of Oncology, University of Cambridge, UK (DEN); Departments of Laboratory Medicine (Clinical Chemistry Service) and Medicine (Genitourinary Oncology Service), Memorial Sloan Kettering Cancer Center, New York, NY (HL); Department of Laboratory Medicine and Clinical Sciences in Malmö, Lund University, Skåne University Hospital, Malmö, Sweden; and Institute of Biomedical Technology, University of Tampere, Finland (HL).
J Natl Cancer Inst. 2015 Apr 11;107(7). doi: 10.1093/jnci/djv095. Print 2015 Jul.
Many men with elevated prostate-specific antigen (PSA) levels in serum do not have aggressive prostate cancer and undergo unnecessary biopsy. Retrospective studies using cryopreserved serum suggest that four kallikrein markers can predict biopsy outcome.
Free, intact and total PSA, and kallikrein-related peptidase 2 were measured in cryopreserved blood from 6129 men with elevated PSA (≥3.0ng/mL) participating in the prospective, randomized trial Prostate Testing for Cancer and Treatment. Marker levels from 4765 men providing anticoagulated plasma were incorporated into statistical models to predict any-grade and high-grade (Gleason score ≥7) prostate cancer at 10-core biopsy. The models were corrected for optimism by 10-fold cross validation and independently validated using markers measured in serum from 1364 men. All statistical tests were two-sided.
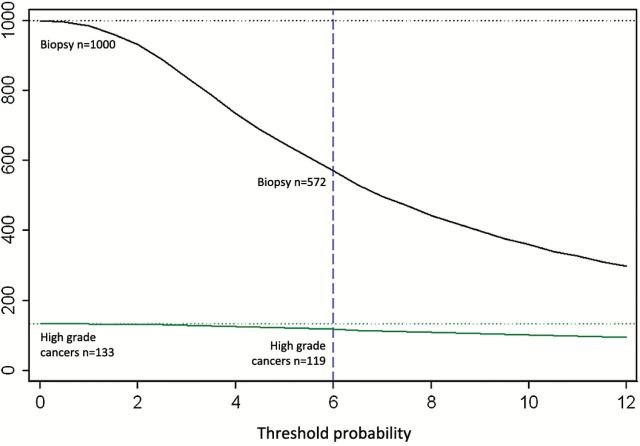
The four kallikreins enhanced prostate cancer detection compared with PSA and age alone. Area under the curve (AUC) for the four kallikreins was 0.719 (95% confidence interval [CI] = 0.704 to 0.734) vs 0.634 (95% CI = 0.617 to 0.651, P < .001) for PSA and age alone for any-grade cancer, and 0.820 (95% CI = 0.802 to 0.838) vs 0.738 (95% CI = 0.716 to 0.761) for high-grade cancer. Using a 6% risk of high-grade cancer as an illustrative cutoff, for 1000 biopsied men with PSA levels of 3.0ng/mL or higher, the model would reduce the need for biopsy in 428 men, detect 119 high-grade cancers, and delay diagnosis of 14 of 133 high-grade cancers. Models exhibited excellent discrimination on independent validation among men with only serum samples available for analysis.
A statistical model based on kallikrein markers was validated in a large prospective study and reduces unnecessary biopsies while delaying diagnosis of high-grade cancers in few men.
许多血清前列腺特异性抗原(PSA)水平升高的男性并没有侵袭性前列腺癌,却接受了不必要的活检。使用冷冻保存血清的回顾性研究表明,四种激肽释放酶标志物可以预测活检结果。
在参与前瞻性随机试验“前列腺癌检测与治疗”的6129名PSA水平升高(≥3.0ng/mL)的男性的冷冻血液中,检测游离、完整和总PSA以及激肽释放酶相关肽酶2。将4765名提供抗凝血浆的男性的标志物水平纳入统计模型,以预测10针活检时任何分级和高级别(Gleason评分≥7)前列腺癌的发生情况。通过10倍交叉验证对模型的乐观性进行校正,并使用在1364名男性血清中测得的标志物进行独立验证。所有统计检验均为双侧检验。
与单独使用PSA和年龄相比,四种激肽释放酶增强了前列腺癌的检测能力。对于任何分级的癌症,四种激肽释放酶的曲线下面积(AUC)为0.719(95%置信区间[CI]=0.704至0.734),而单独使用PSA和年龄时为0.634(95%CI=0.617至0.651,P<.001);对于高级别癌症,AUC为0.820(95%CI=0.802至0.838),而单独使用PSA和年龄时为0.738(95%CI=0.716至0.761)。以6%的高级别癌症风险作为说明性临界值,对于1000名PSA水平为3.0ng/mL或更高的接受活检的男性,该模型将减少428名男性的活检需求,检测出119例高级别癌症,并延迟133例高级别癌症中14例的诊断。在仅可获得血清样本进行分析的男性中,模型在独立验证时表现出出色的区分能力。
基于激肽释放酶标志物的统计模型在一项大型前瞻性研究中得到验证,可减少不必要的活检,同时仅在少数男性中延迟高级别癌症的诊断。