Academic Urology Unit and Institute for Cancer Studies, University of Sheffield, Sheffield, UK.
Br J Cancer. 2011 Sep 27;105(7):931-7. doi: 10.1038/bjc.2011.314. Epub 2011 Aug 23.
Contemporary screening for prostate cancer frequently identifies small volume, low-grade lesions. Some clinicians have advocated focal prostatic ablation as an alternative to more aggressive interventions to manage these lesions. To identify which patients might benefit from focal ablative techniques, we analysed the surgical specimens of a large sample of population-detected men undergoing radical prostatectomy as part of a randomised clinical trial.
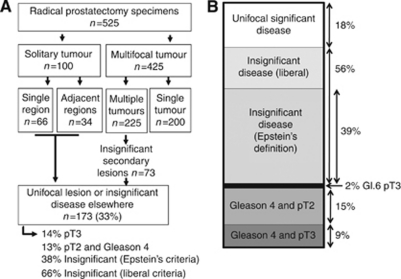
Surgical specimens from 525 men who underwent prostatectomy within the ProtecT study were analysed to determine tumour volume, location and grade. These findings were compared with information available in the biopsy specimen to examine whether focal therapy could be provided appropriately.
Solitary cancers were found in prostatectomy specimens from 19% (100 out of 525) of men. In addition, 73 out of 425 (17%) men had multiple cancers with a solitary significant tumour focus. Thus, 173 out of 525 (33%) men had tumours potentially suitable for focal therapy. The majority of these were small, well-differentiated lesions that appeared to be pathologically insignificant (38-66%). Criteria used to select patients for focal prostatic ablation underestimated the cancer's significance in 26% (34 out of 130) of men and resulted in overtreatment in more than half. Only 18% (24 out of 130) of men presumed eligible for focal therapy, actually had significant solitary lesions.
Focal therapy appears inappropriate for the majority of men presenting with prostate-specific antigen-detected localised prostate cancer. Unifocal prostate cancers suitable for focal ablation are difficult to identify pre-operatively using biopsy alone. Most lesions meeting criteria for focal ablation were either more aggressive than expected or posed little threat of progression.
当代前列腺癌筛查常能发现小体积、低级别病变。一些临床医生主张采用前列腺局部消融术作为更积极干预措施的替代方法来治疗这些病变。为了确定哪些患者可能从局部消融技术中获益,我们分析了一项随机临床试验中接受根治性前列腺切除术的大量人群检测男性的手术标本。
分析 ProtecT 研究中 525 例接受前列腺切除术男性的手术标本,以确定肿瘤体积、位置和分级。将这些发现与活检标本中的信息进行比较,以检查是否可以适当提供局部治疗。
在 525 例男性的前列腺切除标本中发现 19%(100 例)有单发癌。此外,425 例中有 73 例(17%)男性有多发性癌,其中只有一个显著肿瘤焦点。因此,525 例中有 173 例(33%)男性的肿瘤可能适合局部治疗。这些肿瘤大多数为小而分化良好的病变,似乎在病理上无足轻重(38-66%)。用于选择接受前列腺局部消融术的患者的标准低估了癌症在 26%(34 例)男性中的重要性,并导致超过一半的过度治疗。只有 18%(24 例)被认为有资格接受局部治疗的男性实际上有明显的单发病变。
局部治疗似乎不适合大多数因前列腺特异性抗原检测到局限性前列腺癌而就诊的男性。使用单独的活检难以在术前识别适合局部消融的单灶性前列腺癌。符合局部消融标准的大多数病变要么比预期更具侵袭性,要么对进展的威胁较小。