Kim Yong-Hyub, Song Sang-Yun, Shim Hyun-Jeong, Chung Woong-Ki, Ahn Sung-Ja, Yoon Mee Sun, Jeong Jae-Uk, Song Ju-Young, Nam Taek-Keun
Department of Radiation Oncology, Chonnam National University Medical School, Gwangju, Korea.
Department of Thoracic and Cardiovascular Surgery, Chonnam National University Medical School, Gwangju, Korea.
Radiat Oncol J. 2015 Mar;33(1):12-20. doi: 10.3857/roj.2015.33.1.12. Epub 2015 Mar 31.
To evaluate treatment outcomes and determine prognostic factors in patients with esophageal cancer treated with esophagectomy after neoadjuvant chemoradiotherapy (NCRT).
We retrospectively evaluated 39 patients with esophageal cancer who underwent concurrent chemoradiotherapy followed by esophagectomy between 2002 and 2012. Initial clinical stages of patients were stage IB in 1 patient (2.6%), stage II in 5 patients (12.9%), and stage III in 33 patients (84.6%).
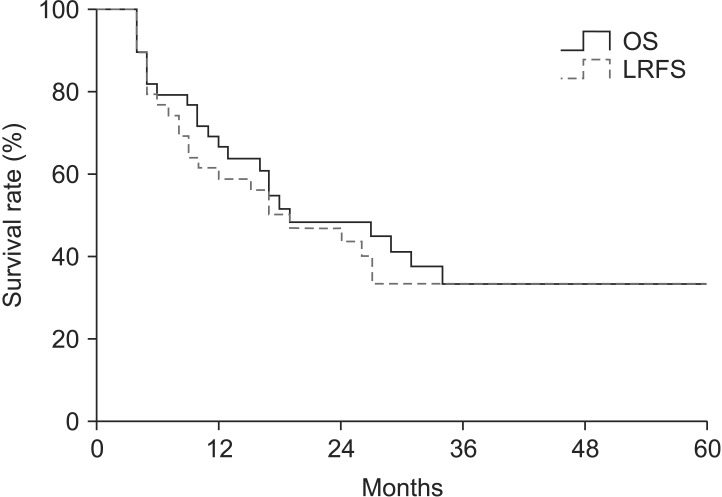
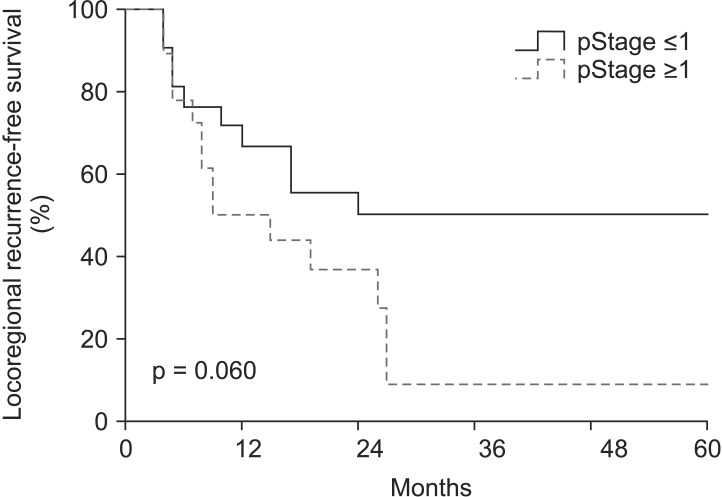
The median age of all the patients was 62 years, and the median follow-up period was 17 months. The 3-year overall survival (OS) rate was 33.6% in all the patients. The 3-year locoregional recurrence-free survival (LRFS) rate was 33.7%. In multivariate analysis with covariates of age, the Eastern Cooperative Oncology Group performance status, hypertension, diabetes mellitus, tumor length, clinical response, clinical stage, pathological response, pathological stage, lymphovascular invasion, surgical type, and radiotherapy to surgery interval, only pathological stage was an independent significant prognostic factor affecting both OS and LRFS. The complications in postoperative day 90 were pneumonia in 9 patients, anastomotic site leakage in 3 patients, and anastomotic site stricture in 2 patients. Postoperative 30-day mortality rate was 10.3% (4/39); the cause of death among these 4 patients was respiratory failure in 3 patients and myocardial infarction in one patient.
Only pathological stage was an independent prognostic factor for both OS and LRFS in patients with esophageal cancer treated with esophagectomy after NCRT. We could confirm the significant role of NCRT in downstaging the initial tumor bulk and thus resulting in better survival of patients who gained earlier pathological stage after NCRT.
评估新辅助放化疗(NCRT)后行食管切除术的食管癌患者的治疗效果,并确定预后因素。
我们回顾性评估了2002年至2012年间39例行同步放化疗后再行食管切除术的食管癌患者。患者的初始临床分期为:1例(2.6%)为ⅠB期,5例(12.9%)为Ⅱ期,33例(84.6%)为Ⅲ期。
所有患者的中位年龄为62岁,中位随访期为17个月。所有患者的3年总生存率(OS)为33.6%。3年局部区域无复发生存率(LRFS)为33.7%。在对年龄、东部肿瘤协作组体能状态、高血压、糖尿病、肿瘤长度、临床反应、临床分期、病理反应、病理分期、淋巴管浸润、手术类型以及放疗至手术间隔时间等协变量进行多因素分析时,只有病理分期是影响OS和LRFS的独立显著预后因素。术后90天内的并发症包括9例肺炎、3例吻合口漏和2例吻合口狭窄。术后30天死亡率为10.3%(4/39);这4例患者的死亡原因是3例呼吸衰竭和1例心肌梗死。
在NCRT后行食管切除术的食管癌患者中,只有病理分期是OS和LRFS的独立预后因素。我们可以证实NCRT在降低初始肿瘤体积方面的重要作用,从而使NCRT后病理分期较早的患者生存率更高。