Masukume Gwinyai, Khashan Ali S, Kenny Louise C, Baker Philip N, Nelson Gill
School of Public Health, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa.
Irish Centre for Fetal and Neonatal Translational Research (INFANT), Department of Obstetrics and Gynaecology, University College Cork, Cork, Ireland; Department of Epidemiology and Public Health, University College Cork, Cork, Ireland.
PLoS One. 2015 Apr 15;10(4):e0122729. doi: 10.1371/journal.pone.0122729. eCollection 2015.
Anaemia in pregnancy is a major public health and economic problem worldwide, that contributes to both maternal and fetal morbidity and mortality.
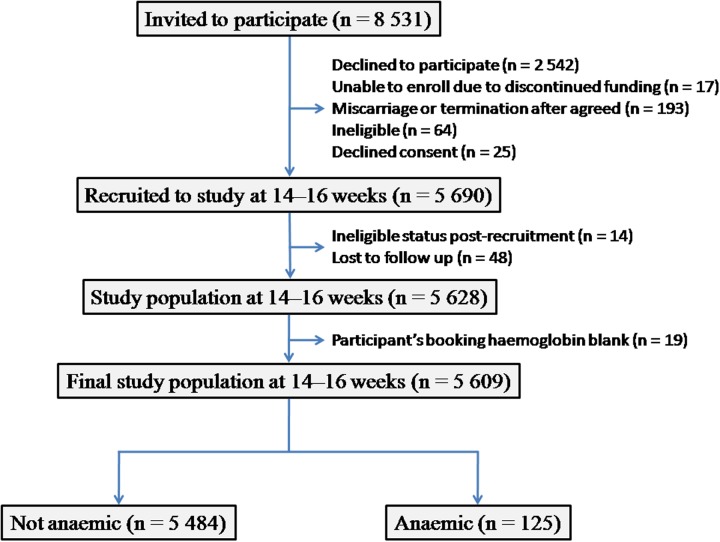
The aim of the study was to calculate the prevalence of anaemia in early pregnancy in a cohort of 'low risk' women participating in a large international multicentre prospective study (n = 5 609), to identify the modifiable risk factors for anaemia in pregnancy in this cohort, and to compare the birth outcomes between pregnancies with and without anaemia in early gestation.
The study is an analysis of data that were collected prospectively during the Screening for Pregnancy Endpoints study. Anaemia was defined according to the World Health Organization's definition of anaemia in pregnancy (haemoglobin < 11g/dL). Binary logistic regression with adjustment for potential confounders (country, maternal age, having a marital partner, ethnic origin, years of schooling, and having paid work) was the main method of analysis.
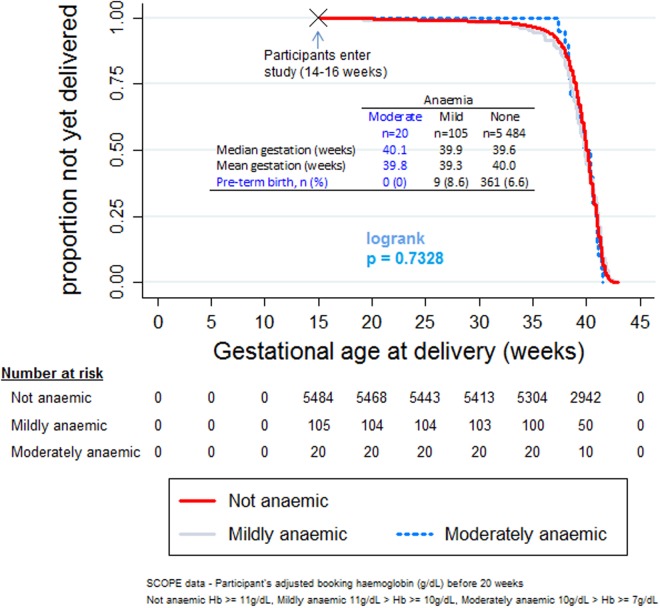
The hallmark findings were the low prevalence of anaemia (2.2%), that having no marital partner was an independent risk factor for having anaemia (OR 1.34, 95% CI 1.01-1.78), and that there was no statistically significant effect of anaemia on adverse pregnancy outcomes (small for gestational age, pre-tem birth, mode of delivery, low birth weight, APGAR score < 7 at one and five minutes). Adverse pregnancy outcomes were however more common in those with anaemia than in those without.
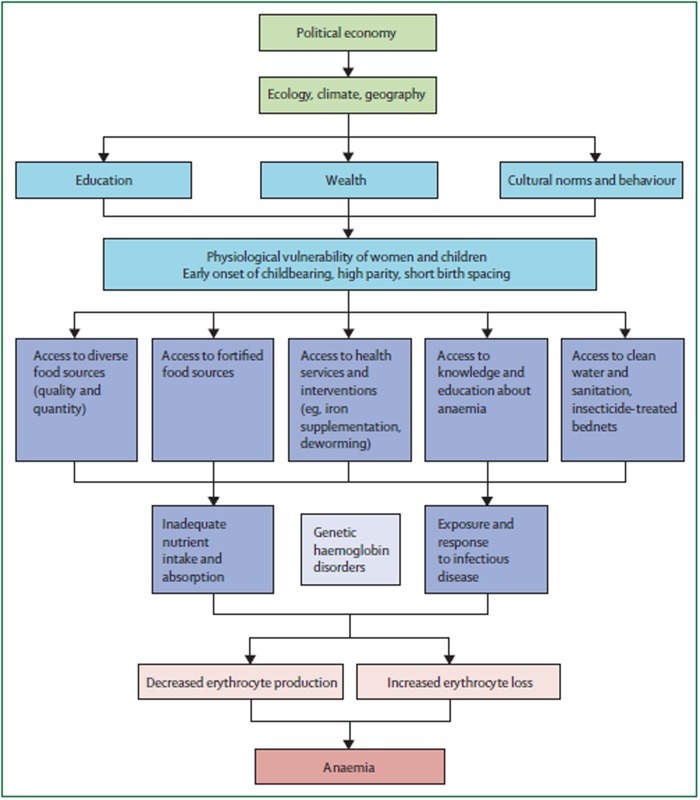
In this low risk healthy pregnant population we found a low anaemia rate. The absence of a marital partner was a non-modifiable factor, albeit one which may reflect a variety of confounding factors, that should be considered for addition to anaemia's conceptual framework of determinants. Although not statistically significant, clinically, a trend towards a higher risk of adverse pregnancy outcomes was observed in women that were anaemic in early pregnancy.
孕期贫血是一个全球性的重大公共卫生和经济问题,会导致孕产妇和胎儿发病及死亡。
本研究旨在计算参与一项大型国际多中心前瞻性研究(n = 5609)的“低风险”女性队列中孕早期贫血的患病率,确定该队列中孕期贫血的可改变风险因素,并比较孕早期有无贫血的妊娠分娩结局。
本研究分析了在妊娠结局筛查研究期间前瞻性收集的数据。贫血根据世界卫生组织对孕期贫血的定义(血红蛋白<11g/dL)来定义。主要分析方法是二元逻辑回归,并对潜在混杂因素(国家、产妇年龄、有配偶、种族、受教育年限和有带薪工作)进行调整。
标志性发现是贫血患病率较低(2.2%),没有配偶是患贫血的独立风险因素(比值比1.34,95%置信区间1.01 - 1.78),且贫血对不良妊娠结局(小于胎龄、早产、分娩方式、低出生体重、1分钟和5分钟时阿氏评分<7)无统计学显著影响。然而,贫血者的不良妊娠结局比无贫血者更常见。
在这个低风险的健康孕妇群体中,我们发现贫血率较低。没有配偶是一个不可改变的因素,尽管它可能反映了多种混杂因素,在贫血决定因素的概念框架中应考虑将其纳入。虽然无统计学显著差异,但临床上观察到孕早期贫血女性不良妊娠结局风险有升高趋势。