Conroy Andrea L, Hawkes Michael, Hayford Kyla, Namasopo Sophie, Opoka Robert O, John Chandy C, Liles W Conrad, Kain Kevin C
Depatment of Medicine, University of Toronto, Toronto, M5S1A8, Canada.
Sandra A. Rotman Laboratories, Sandra Rotman Centre for Global Health, University Health Network-Toronto General Hospital, University of Toronto, Toronto, M5G1L7, Canada.
Crit Care. 2015 Feb 23;19(1):47. doi: 10.1186/s13054-015-0773-4.
The development of simple clinical tools to identify children at risk of death would enable rapid and rational implementation of lifesaving measures to reduce childhood mortality globally.
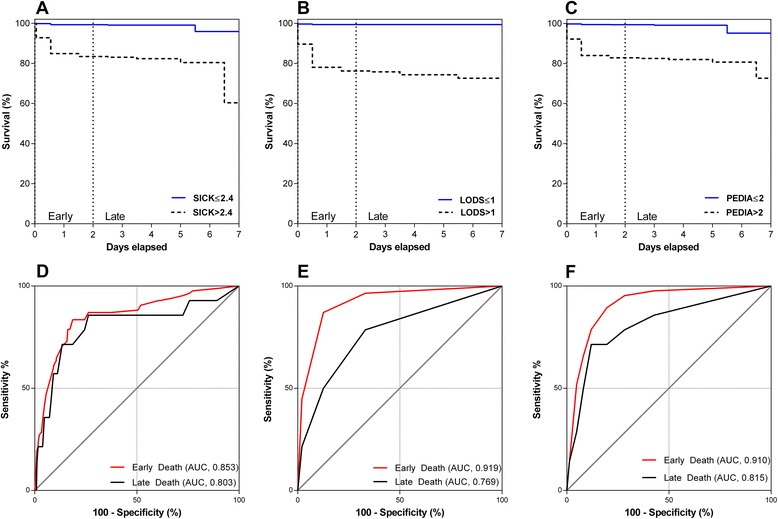
We evaluated the ability of three clinical scoring systems to predict in-hospital mortality in a prospective observational study of Ugandan children with fever. We computed the Lambaréné Organ Dysfunction Score (LODS), Signs of Inflammation in Children that Kill (SICK), and the Pediatric Early Death Index for Africa (PEDIA). Model discrimination was evaluated by comparing areas under receiver operating characteristic curves (AUCs) and calibration was assessed using the Hosmer-Lemeshow goodness-of-fit test. Sub-analyses were performed in malaria versus non-malaria febrile illness (NMFI), and in early (≤48 hours) versus late (>48 hours) deaths.
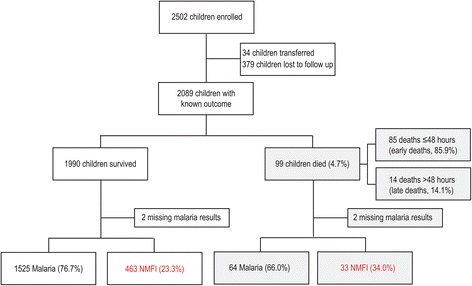
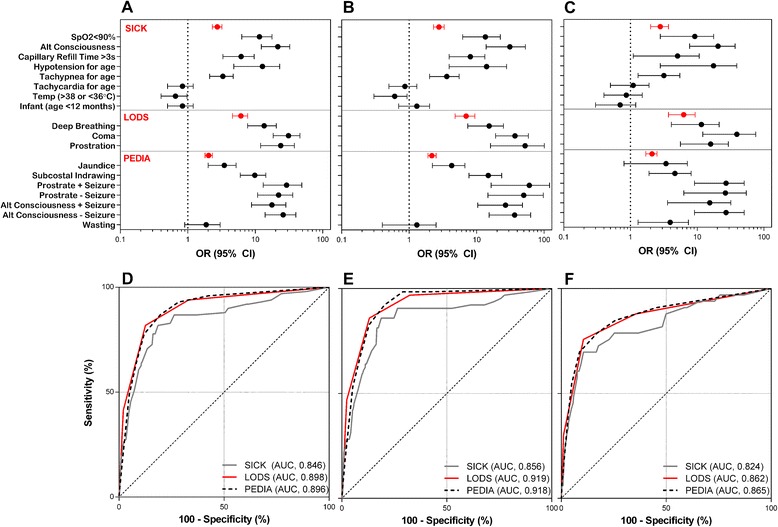
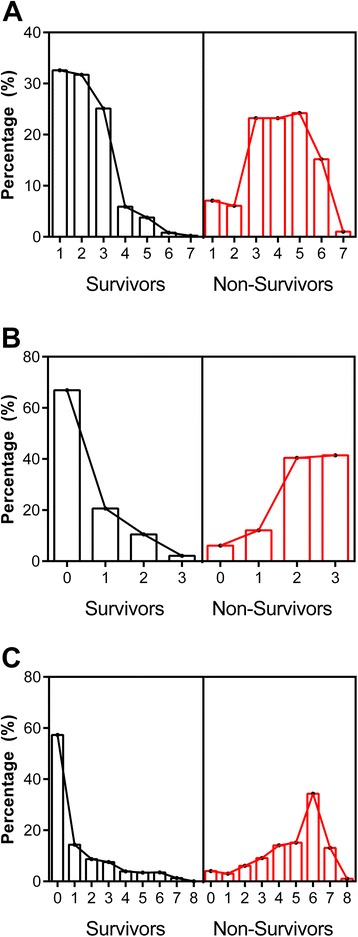
In total, 2089 children with known outcomes were included in the study (99 deaths, 4.7% mortality). All three scoring systems yielded good discrimination (AUCs, 95% confidence interval (CI): LODS, 0.90, 0.88 to 0.91; SICK, 0.85, 0.83 to 0.86; PEDIA, 0.90, 0.88 to 0.91). Using the Youden index to identify the best cut-offs, LODS had the highest positive likelihood ratio (+LR, 95% CI: LODS, 6.5, 5.6 to 7.6; SICK, 4.4, 3.9 to 5.0; PEDIA, 4.4, 3.9 to 5.0), whereas PEDIA had the lowest negative likelihood ratio (-LR, 95% CI: LODS, 0.21, 0.1 to 0.3; SICK, 0.22, 0.1 to 0.3; PEDIA, 0.16, 0.1 to 0.3), LODS and PEDIA were well calibrated (P = 0.79 and P = 0.21 respectively), and had higher AUCs than SICK in discriminating between survivors and non-survivors in malaria (AUCs, 95% CI: LODS, 0.92, 0.90 to 0.93; SICK, 0.86, 0.84 to 0.87; PEDIA, 0.92, 0.90 to 0.93), but comparable AUCs in NMFI (AUCs, 95% CI: LODS, 0.86, 0.83 to 0.89; SICK, 0.82, 0.79 to 0.86; PEDIA, 0.87, 0.83 to 0.893). The majority of deaths in the study occurred early (n = 85, 85.9%) where LODS and PEDIA had good discrimination.
All three scoring systems predicted outcome, but LODS holds the most promise as a clinical prognostic score based on its simplicity to compute, requirement for no equipment, and good discrimination.
开发简单的临床工具以识别有死亡风险的儿童,将有助于迅速且合理地实施挽救生命的措施,从而降低全球儿童死亡率。
在一项针对乌干达发热儿童的前瞻性观察研究中,我们评估了三种临床评分系统预测住院死亡率的能力。我们计算了兰巴雷内器官功能障碍评分(LODS)、儿童致死性炎症体征(SICK)以及非洲儿科早期死亡指数(PEDIA)。通过比较受试者工作特征曲线下面积(AUC)来评估模型的辨别力,并使用霍斯默 - 莱梅肖拟合优度检验评估校准情况。在疟疾与非疟疾发热性疾病(NMFI)以及早期(≤48小时)与晚期(>48小时)死亡情况中进行了亚组分析。
该研究共纳入2089名已知结局的儿童(99例死亡,死亡率4.7%)。所有三种评分系统都具有良好的辨别力(AUC,95%置信区间(CI):LODS为0.90,0.88至0.91;SICK为0.85,0.83至0.86;PEDIA为0.90,0.88至0.91)。使用约登指数确定最佳临界值时,LODS具有最高的阳性似然比(+LR,95%CI:LODS为6.5,5.6至7.6;SICK为4.4,3.9至5.0;PEDIA为4.4,3.9至5.0),而PEDIA具有最低的阴性似然比(-LR,95%CI:LODS为0.21,0.1至0.3;SICK为0.22,0.1至0.3;PEDIA为0.16,0.1至0.3),LODS和PEDIA校准良好(分别为P = 0.79和P = 0.21),并且在区分疟疾患者的存活者和非存活者方面,LODS和PEDIA的AUC高于SICK(AUC,95%CI:LODS为0.92,0.90至0.93;SICK为0.86,0.84至0.87;PEDIA为0.92,0.90至0.93),但在NMFI中AUC相当(AUC,95%CI:LODS为0.86,0.83至0.89;SICK为0.82,0.79至0.86;PEDIA为0.87,0.83至0.893)。研究中的大多数死亡发生在早期(n = 85,85.9%),此时LODS和PEDIA具有良好的辨别力。
所有三种评分系统都能预测结局,但基于其计算简单、无需设备且辨别力良好,LODS作为临床预后评分最具前景。