Department of Radiation Oncology, The Ohio State University James Cancer Hospital, The Ohio State University Wexner Medical Center, Columbus, Ohio, 43210, United States of America.
Department of Radiation Oncology, University of Virginia Health System, Charlottesville, Virginia, 22903, United States of America.
PLoS One. 2015 Apr 20;10(4):e0126222. doi: 10.1371/journal.pone.0126222. eCollection 2015.
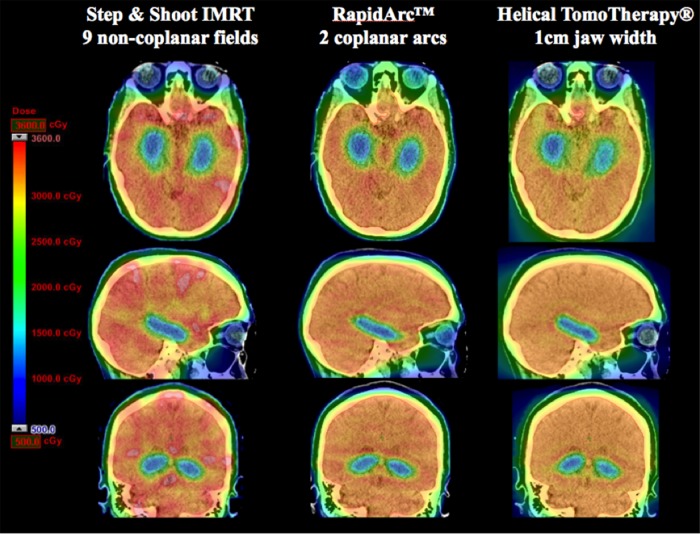
Whole brain radiotherapy (WBRT) is a vital tool in radiation oncology and beyond, but it can result in adverse health effects such as neurocognitive decline. Hippocampal Avoidance WBRT (HA-WBRT) is a strategy that aims to mitigate the neuro-cognitive side effects of whole brain radiotherapy treatment by sparing the hippocampi while delivering the prescribed dose to the rest of the brain. Several competing modalities capable of delivering HA-WBRT, include: Philips Pinnacle step-and-shoot intensity modulated radiotherapy (IMRT), Varian RapidArc volumetric modulated arc therapy (RapidArc), and helical TomoTherapy (TomoTherapy).
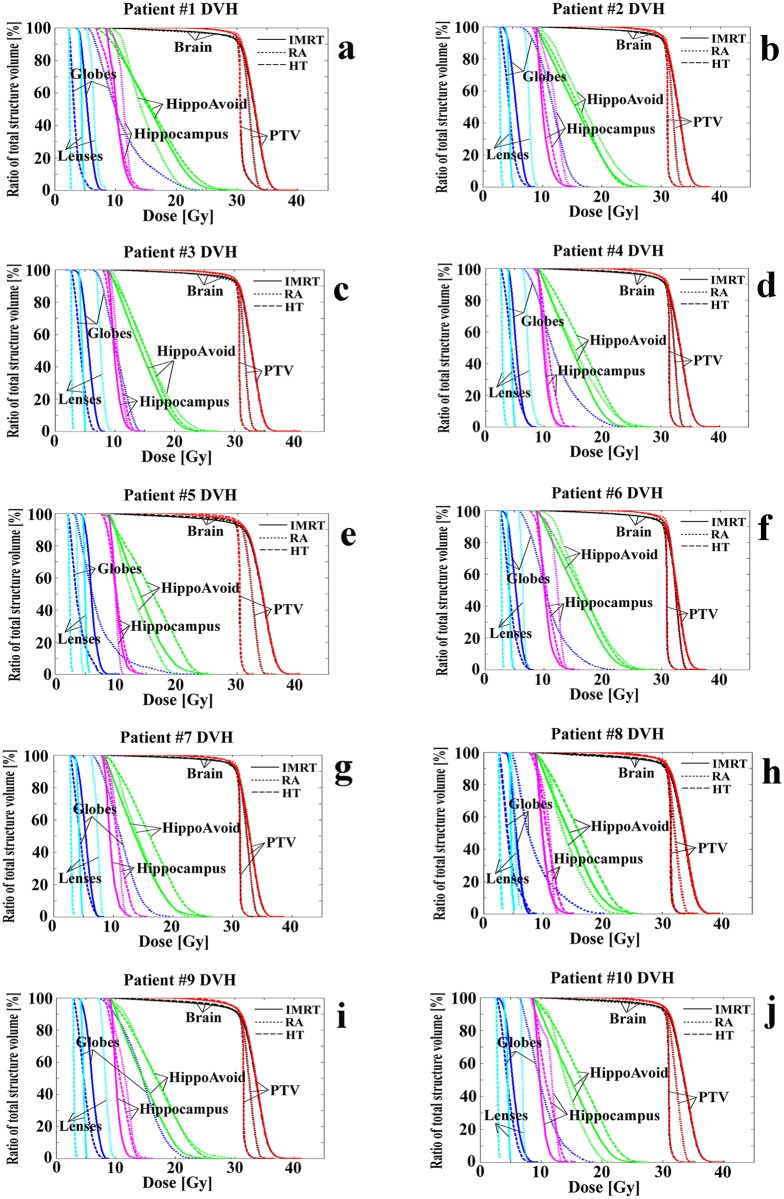
In this study we compared these methods using 10 patient datasets. Anonymized planning CT (computerized tomography) scans and contour data based on fused MRI images were collected. Three independent planners generated treatment plans for the patients using three modalities, respectively. All treatment plans met the RTOG 0933 criteria for HA-WBRT treatment.
In dosimetric comparisons between the three modalities, TomoTherapy has a significantly superior homogeneity index of 0.15 ± 0.03 compared to the other two modalities (0.28 ± .04, p < .005 for IMRT and 0.22 ± 0.03, p < .005 for RapidArc). RapidArc has the fastest average delivery time of 2.5 min compared to the other modalities (15 min for IMRT and 18 min for TomoTherapy).
TomoTherapy is considered to be the preferred modality for HA-WBRT due to its superior dose distribution. When TomoTherapy is not available or treatment time is a concern, RapidArc can provide sufficient dose distribution meeting RTOG criteria and efficient treatment delivery.
全脑放疗(WBRT)是放射肿瘤学等领域的重要工具,但它会导致神经认知功能下降等不良健康影响。海马回避全脑放疗(HA-WBRT)是一种策略,旨在通过在给予大脑其余部分规定剂量的同时保护海马,来减轻全脑放疗治疗的神经认知副作用。有几种能够提供 HA-WBRT 的竞争方式,包括:飞利浦 Pinnacle 步进和射击强度调制放疗(IMRT)、瓦里安 RapidArc 容积调制弧形治疗(RapidArc)和螺旋 TomoTherapy(TomoTherapy)。
在这项研究中,我们使用了 10 个患者数据集来比较这些方法。收集了匿名的计划 CT(计算机断层扫描)扫描和基于融合 MRI 图像的轮廓数据。三位独立的规划师分别使用三种方式为患者生成治疗计划。所有的治疗计划都符合 RTOG 0933 的 HA-WBRT 治疗标准。
在三种方式的剂量学比较中,与其他两种方式相比,TomoTherapy 的均匀性指数具有明显优势,为 0.15±0.03,而其他两种方式分别为 0.28±0.04(p<0.005 与 IMRT 相比)和 0.22±0.03(p<0.005 与 RapidArc 相比)。RapidArc 的平均治疗时间最快,为 2.5 分钟,而其他两种方式分别为 15 分钟(IMRT)和 18 分钟(TomoTherapy)。
由于其优越的剂量分布,TomoTherapy 被认为是 HA-WBRT 的首选方式。当 TomoTherapy 不可用时或治疗时间是一个问题时,RapidArc 可以提供足够的满足 RTOG 标准的剂量分布和高效的治疗输送。