Eklund Anton, Slettengren Martin, van der Linden Jan
Department of Cardiothoracic Surgery and Anesthesiology, Karolinska University Hospital, SE-17176, Stockholm, Sweden.
Department of Molecular Medicine and Surgery, Karolinska Institutet, SE-17177, Stockholm, Sweden.
Crit Care. 2015 Apr 21;19(1):173. doi: 10.1186/s13054-015-0899-4.
In the intensive care setting, most physiologic parameters are monitored automatically. However, urine output (UO) is still monitored hourly by manually handled urinometers. In this study, we evaluated an automatic urinometer (AU) and compared it with a manual urinometer (MU).
This prospective study was carried out in the intensive care unit of a cardiothoracic surgical clinic. In postoperative patients (n = 34) with indwelling urinary catheters and an expected stay of 24 hours or more, hourly UO samples were measured with an AU (Sippi, n = 220; Observe Medical, Gothenburg, Sweden) or an MU (UnoMeter™ 500, n = 188; Unomedical, Birkerød, Denmark) and thereafter validated by cylinder measurements. Malposition of the instrument at the time of reading excluded measurement. Data were analyzed with the Bland-Altman method. The performance of the MU was used as the minimum criterion of acceptance when the AU was evaluated. The loss of precision with the MU due to temporal deviation from fixed hourly measurements was recorded (n = 108). A questionnaire filled out by the ward staff (n = 28) was used to evaluate the ease of use of the AU compared with the MU.
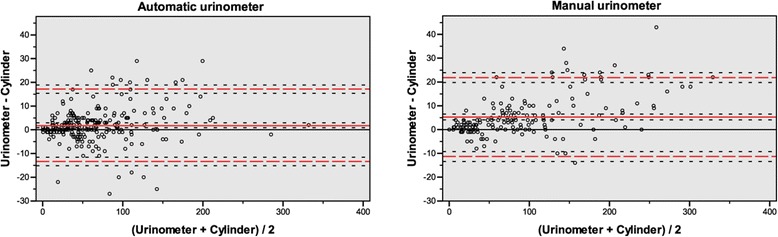
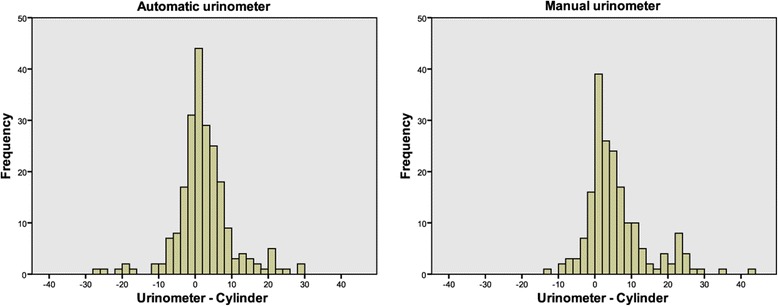
Bland-Altman analysis showed a smaller mean bias for the AU (+1.9 ml) compared with the MU (+5.3 ml) (P <0.0001). There was no statistical difference in measurement precision between the two urinometers, as defined by their limits of agreement (±15.2 ml vs. ±16.6 ml, P = 0.11). The mean temporal variation with the MU was ±7.4 minutes (±12.4%), and the limits of agreement were ±23.9 minutes (±39.8%), compared with no temporal variation with the AU (P <0.0001). The ward staff considered the AU easy to learn to use and rated it higher than the MU (P <0.0001).
The AU was not inferior to the MU and was significantly better in terms of bias, temporal deviation and staff opinion, although the clinical relevance of these findings may be open to discussion.
在重症监护环境中,大多数生理参数都是自动监测的。然而,尿量(UO)仍需通过人工操作的尿比重计每小时监测一次。在本研究中,我们评估了一种自动尿比重计(AU),并将其与手动尿比重计(MU)进行了比较。
这项前瞻性研究在一家心胸外科诊所的重症监护病房进行。对术后留置导尿管且预计住院时间为24小时或更长时间的患者(n = 34),每小时采集的尿量样本用AU(Sippi,n = 220;瑞典哥德堡的Observe Medical公司)或MU(UnoMeter™ 500,n = 188;丹麦比克勒的Unomedical公司)进行测量,然后通过量筒测量进行验证。读数时仪器位置不当则排除该测量值。数据采用布兰德 - 奥特曼方法进行分析。评估AU时,以MU的性能作为可接受的最低标准。记录MU因与固定每小时测量时间偏差导致的精度损失(n = 108)。病房工作人员(n = 28)填写的问卷用于评估AU与MU相比的易用性。
布兰德 - 奥特曼分析显示,与MU(平均偏差 +5.3毫升)相比,AU的平均偏差较小(+1.9毫升)(P <0.0001)。根据一致性界限定义,两种尿比重计的测量精度无统计学差异(±15.2毫升对±16.6毫升,P = 0.11)。MU的平均时间变化为±7.4分钟(±12.4%),一致性界限为±23.9分钟(±39.8%),而AU无时间变化(P <0.0001)。病房工作人员认为AU易于学习使用,对其评价高于MU(P <0.0001)。
AU并不逊色于MU,在偏差、时间偏差和工作人员评价方面明显更好,尽管这些发现的临床相关性可能有待讨论。