Niitsu Hiroaki, Hinoi Takao, Shimomura Manabu, Egi Hiroyuki, Hattori Minoru, Ishizaki Yasuyo, Adachi Tomohiro, Saito Yasufumi, Miguchi Masashi, Sawada Hiroyuki, Kochi Masatoshi, Mukai Shoichiro, Ohdan Hideki
Department of Gastroenterological and Transplant Surgery, Applied Life Sciences, Institute of Biomedical & Health Sciences, Hiroshima University, 1-2-3 Kasumi, Minamiku, Hiroshima, 734-8551, Japan.
World J Surg Oncol. 2015 Apr 24;13:162. doi: 10.1186/s12957-015-0570-1.
In stage IV colorectal cancer (CRC) with unresectable metastases, whether or not resection of the primary tumor should be indicated remains controversial. We aim to determine the impact of primary tumor resection on the survival of stage IV CRC patients with unresectable metastases.
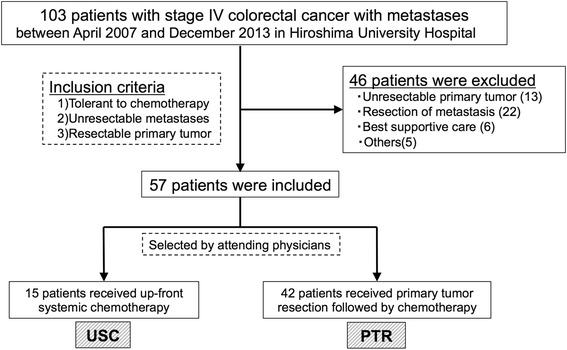
We retrospectively investigated 103 CRC patients with stage IV colorectal cancer with metastases, treated at Hiroshima University Hospital between 2007 and 2013. Of these, those who had resectable primary tumor but unresectable metastases and received any chemotherapy were included in the study. We analyzed the overall survival (OS) and short-term outcomes between the patients who received up-front systemic chemotherapy (USC group) and those who received primary tumor resection followed by chemotherapy (PTR group).
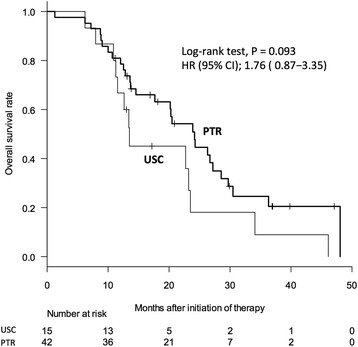
Of the 57 included patients, 15 underwent USC and 42 PTR. The median survival times were 13.4 and 23.9 months in the USC and PTR groups, respectively (P = 0.093), but multivariate analysis for the overall survival showed no significant difference between the two groups (hazard ratio, 1.30; 95% confidence interval (CI), 0.60 to 2.73, P = 0.495). In the USC group, the disease control rate of primary tumor was observed in 12 patients (80.0%), but emergency laparotomy was required for 1 patient. Morbidity in the PTR group was observed in 18 cases (42.9%).
The overall survival did not differ significantly between the USC and PTR groups. USC may help avoid unnecessary resection and consequently the high morbidity rate associated with primary tumor resection for stage IV CRC with unresectable metastases.
在伴有不可切除转移灶的IV期结直肠癌(CRC)中,是否应进行原发肿瘤切除仍存在争议。我们旨在确定原发肿瘤切除对伴有不可切除转移灶的IV期CRC患者生存的影响。
我们回顾性研究了2007年至2013年在广岛大学医院接受治疗的103例伴有转移的IV期结直肠癌患者。其中,那些原发肿瘤可切除但转移灶不可切除且接受过任何化疗的患者被纳入研究。我们分析了接受 upfront 全身化疗的患者(USC组)和接受原发肿瘤切除后化疗的患者(PTR组)之间的总生存期(OS)和短期结局。
在纳入的57例患者中,15例接受了USC,42例接受了PTR。USC组和PTR组的中位生存时间分别为13.4个月和23.9个月(P = 0.093),但总生存期的多因素分析显示两组之间无显著差异(风险比,1.30;95%置信区间(CI),0.60至2.73,P = 0.495)。在USC组中,12例患者(80.0%)观察到原发肿瘤的疾病控制率,但1例患者需要急诊剖腹手术。PTR组有18例(42.9%)出现并发症。
USC组和PTR组的总生存期无显著差异。USC可能有助于避免不必要的切除,从而避免与伴有不可切除转移灶的IV期CRC原发肿瘤切除相关的高发病率。