Jiang Xuqin, Mei Xiaodong, Feng Di, Wang Xiaojing
Department of Respiratory Medicine, Anhui Provincial Hospital, Hefei, China.
PLoS One. 2015 Apr 24;10(4):e0122171. doi: 10.1371/journal.pone.0122171. eCollection 2015.
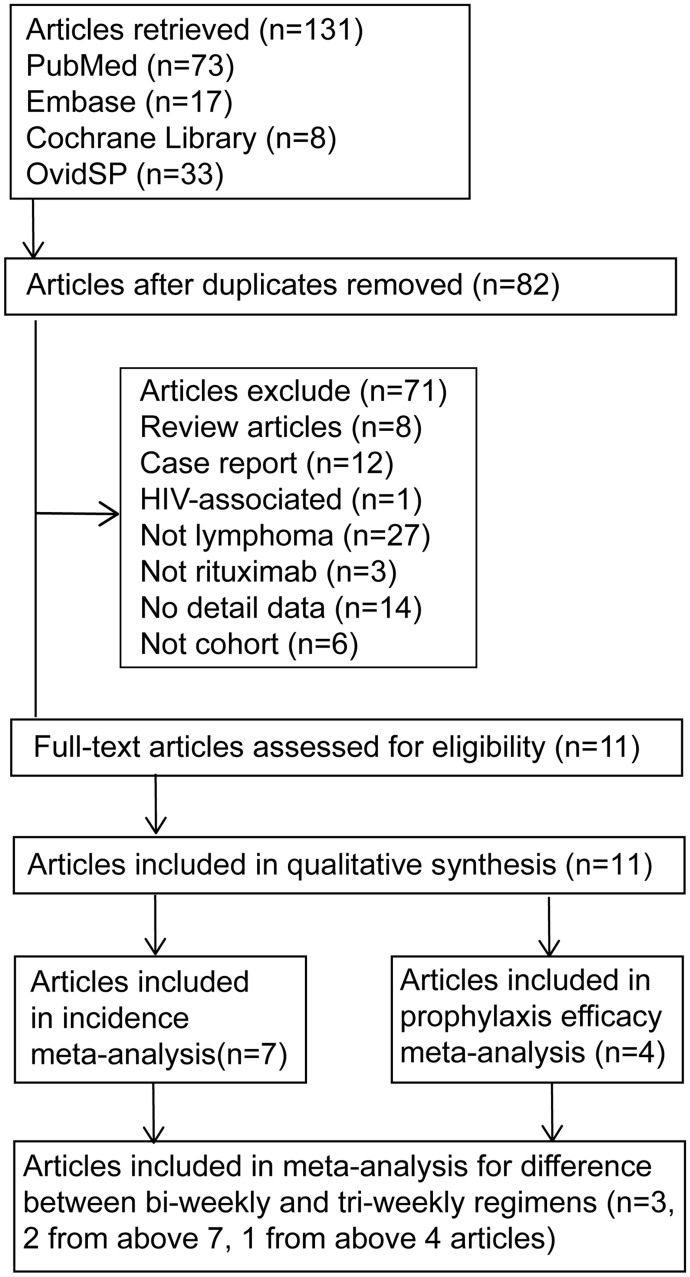
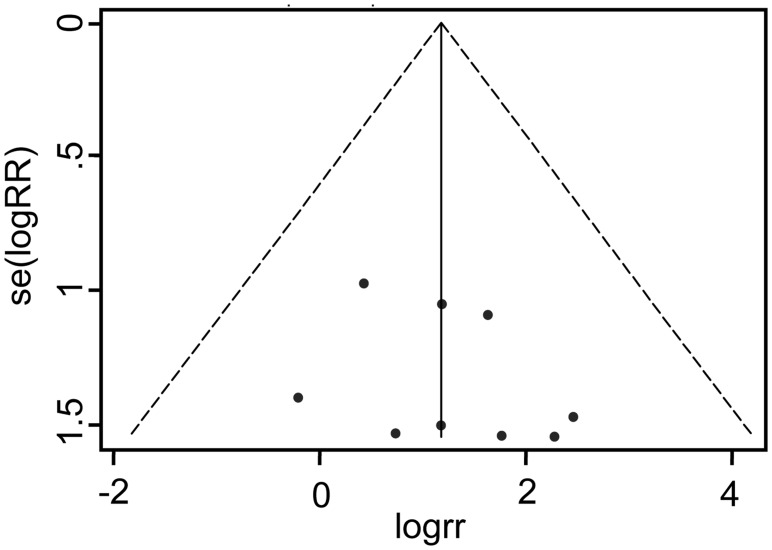
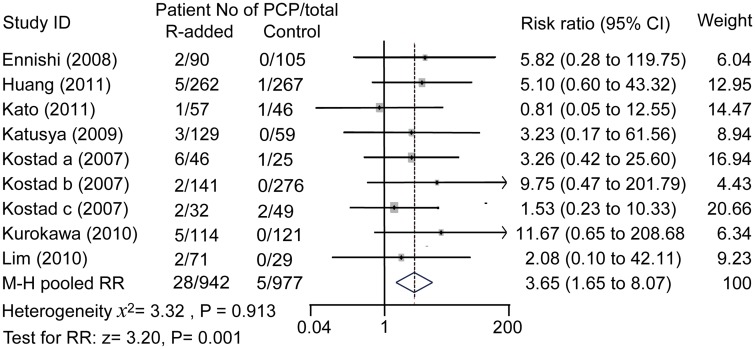
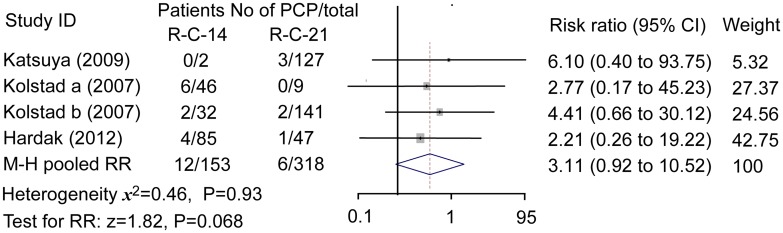
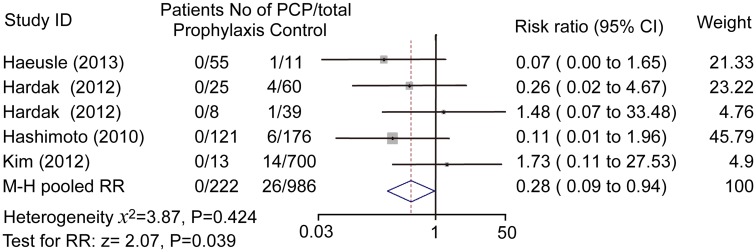
Pneumocystis jiroveci pneumonia (PCP) is frequently reported in lymphoma patients treated with rituximab-contained regimens. There is a trend toward a difference in PCP risk between bi- and tri-weekly regimens. The aims of this systemic review and meta-analysis were to estimate the risk for PCP in these patients, compare the impact of different regimens on the risk, and evaluate the efficacy of prophylaxis. The cohort studies with incept up to January 2014 were retrieved from the Cochrane Library, Medline, Embase, and Web of Science databases. Studies that compared the incidence of PCP in patients with and without rituximab treatment were conducted. Studies that reported the results of prophylaxis were concentrated to evaluate the efficacy of prophylaxis. Fixed effect Mantel-Haenszel model was chosen as the main analysis method. Funnel plots were examined to estimate the potential selection bias. Egger's test and Begg's test were used for the determination of possible small study bias. Eleven cohort studies that met the inclusion criteria were finally included. Results indicated that rituximab was associated with a significantly increased risk for PCP (28/942 vs 5/977; risk ratio: 3.65; 95% confidence interval 1.65 to 8.07; P=0.001), and no heterogeneity existed between different studies (I2=0%). Little significant difference in PCP risk was found between bi-weekly and tri-weekly regimens (risk ratio: 3.11; 95% confidence interval 0.92 to 10.52, P=0.068). PCP risk was inversely associated with prophylaxis in patients treated with rituximab (0/222 vs 26/986; risk ratio: 0.28; 95% confidence interval 0.09 to 0.94; P=0.039). In conclusion, PCP risk was increased significantly in lymphoma patients subjected to rituximab-contained chemotherapies. Difference in PCP risk between bi-weekly and tri-weekly regimens was not significant. Additionally, prophylaxis was dramatically effective in preventing PCP in rituximab-received lymphoma patients, suggesting that rituximab should be recommended for these patients.
接受含利妥昔单抗方案治疗的淋巴瘤患者中,耶氏肺孢子菌肺炎(PCP)的报道屡见不鲜。每两周和每三周治疗方案的PCP风险存在差异趋势。本系统评价和荟萃分析的目的是评估这些患者发生PCP的风险,比较不同方案对风险的影响,并评估预防措施的疗效。检索了截至2014年1月收录于Cochrane图书馆、Medline、Embase和科学网数据库中的队列研究。开展了比较接受和未接受利妥昔单抗治疗患者中PCP发病率的研究。集中分析报告了预防措施结果的研究,以评估预防措施的疗效。选择固定效应Mantel-Haenszel模型作为主要分析方法。通过漏斗图评估潜在的选择偏倚。采用Egger检验和Begg检验确定可能存在的小研究偏倚。最终纳入了11项符合纳入标准的队列研究。结果表明,利妥昔单抗与PCP风险显著增加相关(28/942 vs 5/977;风险比:3.65;95%置信区间1.65至8.07;P = 0.001),不同研究之间不存在异质性(I2 = 0%)。每两周和每三周治疗方案的PCP风险差异无统计学意义(风险比:3.11;95%置信区间0.92至10.52,P = 0.068)。在接受利妥昔单抗治疗的患者中,PCP风险与预防措施呈负相关(0/222 vs 26/986;风险比:0.28;95%置信区间0.09至0.94;P = 0.039)。总之,接受含利妥昔单抗化疗的淋巴瘤患者PCP风险显著增加。每两周和每三周治疗方案的PCP风险差异不显著。此外,预防措施在预防接受利妥昔单抗治疗的淋巴瘤患者发生PCP方面非常有效,提示应对这些患者推荐使用利妥昔单抗。