Gallagher Benjamin D, Muntner Paul, Moise Nathalie, Lin Jenny J, Kronish Ian M
aCenter for Behavioral Cardiovascular Health, Department of Medicine, Columbia University Medical Center, New York, New York bDepartment of Epidemiology, University of Alabama at Birmingham, Birmingham, Alabama cDivision of General Internal Medicine, Icahn School of Medicine at Mount Sinai, New York, New York, USA.
J Hypertens. 2015 May;33(5):1108-13. doi: 10.1097/HJH.0000000000000503.
Medication nonadherence is a major cause of uncontrolled hypertension, but clinicians are poor at judging adherence, and the gold standard for measuring adherence, electronic monitoring, is rarely available in clinical settings. Self-report questionnaires (SRQs), by contrast, are inexpensive, easy to administer, and hence, may be useful for 'diagnosing' nonadherence. In this study, we evaluated the validity of two commonly used medication adherence SRQs among patients with uncontrolled hypertension, using electronic pillbox measurement as the gold standard.
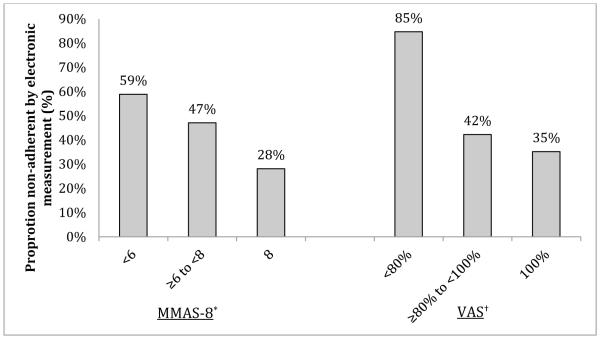
A total of 149 patients with uncontrolled hypertension had adherence to their antihypertensive medication regimen monitored using a four-compartment electronic pillbox (MedSignals) between two primary care visits (median 50 days). Participants completed the 8-item Morisky Medication Adherence Scale (MMAS-8) and the Visual Analog Scale (VAS) at the second visit. Likelihood ratios were calculated using less than 80% correct dosing adherence by electronic measurement as the gold standard.
SRQ scores indicating low adherence (MMAS-8 <6 and VAS <80%, 23 and 9% of participants, respectively) had likelihood ratios of 2.00 [95% confidence interval (CI) 1.10-3.65] and 7.72 (95% CI 1.77-33.6), respectively, for detecting nonadherence compared to electronic measurement. SRQ scores indicating highest adherence (MMAS-8 = 8 and VAS = 100%, 43 and 61% of participants, respectively) had likelihood ratios of 0.55 (95% CI 0.35-0.85) and 0.76 (95% CI 0.57-1.01), respectively, for detecting nonadherence.
The MMAS-8 and VAS are modestly useful in identifying antihypertensive medication nonadherence. Other tools, including electronic measurement, may be needed to guide titration of antihypertensive medications among patients with uncontrolled hypertension.
药物治疗依从性不佳是高血压控制不佳的主要原因,但临床医生在判断依从性方面能力欠佳,而测量依从性的金标准——电子监测,在临床环境中很少可用。相比之下,自我报告问卷(SRQ)价格低廉、易于实施,因此可能有助于“诊断”依从性不佳。在本研究中,我们以电子药盒测量为金标准,评估了两种常用的药物治疗依从性SRQ在高血压控制不佳患者中的有效性。
共有149例高血压控制不佳的患者在两次初级保健就诊期间(中位时间50天)使用四格电子药盒(MedSignals)监测其抗高血压药物治疗方案的依从性。参与者在第二次就诊时完成了8项Morisky药物治疗依从性量表(MMAS-8)和视觉模拟量表(VAS)。以电子测量显示正确给药依从性低于80%作为金标准计算似然比。
表明依从性低的SRQ评分(MMAS-8<6和VAS<80%,分别占参与者的23%和9%),与电子测量相比,检测不依从性的似然比分别为2.00[95%置信区间(CI)1.10 - 3.65]和7.72(95%CI 1.77 - 33.6)。表明依从性最高的SRQ评分(MMAS-8 = 8和VAS = 100%,分别占参与者的43%和61%),检测不依从性的似然比分别为0.55(95%CI 0.35 - 0.85)和0.76(95%CI 0.57 - 1.01)。
MMAS-8和VAS在识别抗高血压药物治疗不依从性方面有一定作用。可能需要其他工具,包括电子测量,来指导高血压控制不佳患者的抗高血压药物滴定。