Chang Hsien-Yen, Zhou Meijia, Tang Wenze, Alexander G Caleb, Singh Sonal
Department of Health Policy and Management, Center for Drug Safety and Effectiveness, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA
Department of Epidemiology, Center for Drug Safety and Effectiveness, Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA.
BMJ. 2015 Apr 24;350:h1585. doi: 10.1136/bmj.h1585.
To determine the real world safety of dabigatran or rivaroxaban compared with warfarin in terms of gastrointestinal bleeding.
Retrospective cohort study.
Large administrative database of commercially insured people in United States from 1 October 2010 through 31 March 2012.
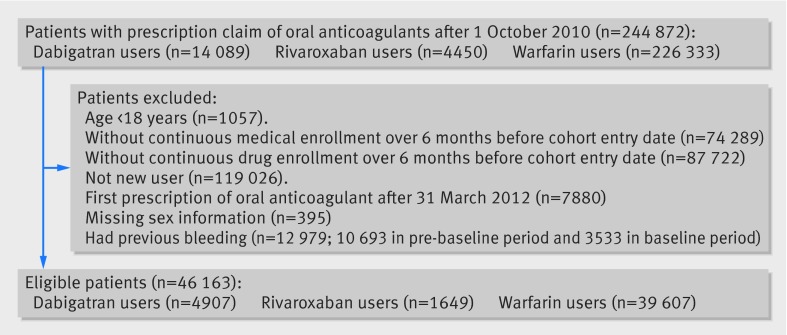
Enrollees with a prescription of warfarin, dabigatran, or rivaroxaban between 1 October 2010 and 31 March 2012, who were aged 18 years or older, had continuous enrollment and no oral anticoagulant use during the six months before the entry date, with known age and sex, and with no gastrointestinal bleeding for at least six months before the cohort entry date. The final study sample of 46,163 patients included 4907 using dabigatran, 1649 using rivaroxaban, and 39,607 using warfarin.
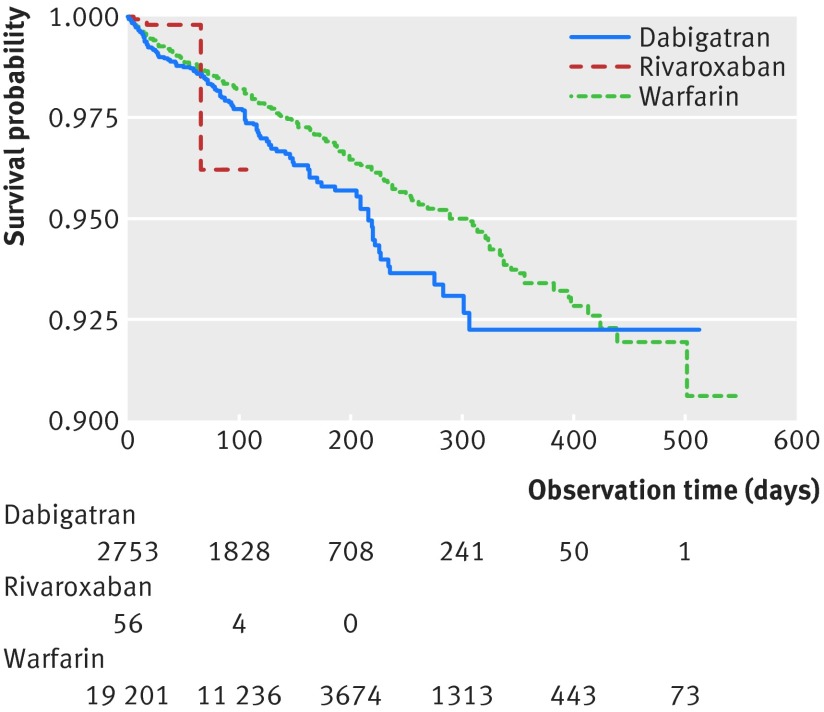
Time to gastrointestinal bleeding. Hazard ratios were derived from Cox proportional hazard models with propensity score weighting and robust estimates of errors.
Dabigatran users tended to be older (dabigatran v rivaroxaban v warfarin: 62.0 v 57.6 v 57.4 years) and more likely to be male (69% v 49% v 53%). The rate of gastrointestinal bleeding was highest among dabigatran users and lowest among rivaroxaban users (dabigatran v rivaroxaban v warfarin: 9.01 v 3.41 v 7.02 cases per 100 person years). After adjustment for potentially confounding covariates, there was no evidence of a statistically significant difference in the risk of gastrointestinal bleeding between dabigatran and warfarin users (adjusted hazard ratio 1.21, 95% confidence interval 0.96 to 1.53) or between rivaroxaban and warfarin users (0.98, 0.36 to 2.69).
Although rates of gastrointestinal bleeding seem to be similar in this commercially insured sample of adults in the United States, we cannot rule out as much as a 50% increase in the risk of gastrointestinal bleeding with dabigatran compared with warfarin or a more than twofold higher risk of bleeding with rivaroxaban compared with warfarin.
比较达比加群或利伐沙班与华法林在胃肠道出血方面的真实世界安全性。
回顾性队列研究。
来自美国2010年10月1日至2012年3月31日商业保险人群的大型管理数据库。
2010年10月1日至2012年3月31日期间开具华法林、达比加群或利伐沙班处方的参保者,年龄在18岁及以上,在入组日期前连续参保且在入组前六个月内未使用口服抗凝剂,已知年龄和性别,且在队列入组日期前至少六个月无胃肠道出血。最终的46163例患者研究样本包括4907例使用达比加群的患者、1649例使用利伐沙班的患者和39607例使用华法林的患者。
胃肠道出血时间。风险比由Cox比例风险模型得出,并采用倾向评分加权和稳健的误差估计。
使用达比加群的患者往往年龄更大(达比加群对比利伐沙班对比华法林:62.0岁对比57.6岁对比57.4岁),且更可能为男性(69%对比49%对比53%)。胃肠道出血发生率在使用达比加群的患者中最高,在使用利伐沙班的患者中最低(达比加群对比利伐沙班对比华法林:每100人年9.01例对比3.41例对比7.02例)。在对潜在混杂协变量进行调整后,没有证据表明使用达比加群的患者与使用华法林的患者在胃肠道出血风险上存在统计学显著差异(调整后的风险比为1.21,95%置信区间为0.96至1.53),也没有证据表明使用利伐沙班的患者与使用华法林的患者在胃肠道出血风险上存在统计学显著差异(0.98,0.36至2.69)。
尽管在美国这个商业保险的成人样本中胃肠道出血发生率似乎相似,但我们不能排除与华法林相比,达比加群导致胃肠道出血风险增加多达50%,或与华法林相比,利伐沙班出血风险高出两倍以上的可能性。