Bateni Sarah B, Meyers Frederick J, Bold Richard J, Canter Robert J
Divison of Surgical Oncology, Department of Surgery, University of California at Davis Medical Center, Sacramento, California.
Division of Hematology/Oncology, Department of Internal Medicine, University of California at Davis Medical Center, Sacramento, California; Vice Dean UC Davis School of Medicine, University of California at Davis Medical Center, California.
J Surg Res. 2015 Jul;197(1):118-25. doi: 10.1016/j.jss.2015.03.063. Epub 2015 Mar 27.
Surgical morbidity and mortality (M&M) for patients with disseminated malignancy (DMa) is high, and some have questioned the role of surgery. Therefore, we sought to characterize temporal trends in M&M among DMa patients, hypothesizing that surgical intervention would remain prevalent.
We queried the American College of Surgeons National Surgical Quality Improvement Program from 2006-2010. Excluding patients undergoing a primary hepatic operation, we identified 21,755 patients with DMa. Parametric and/or nonparametric statistics and logistic regression were used to evaluate temporal trends and predictors of M&M.
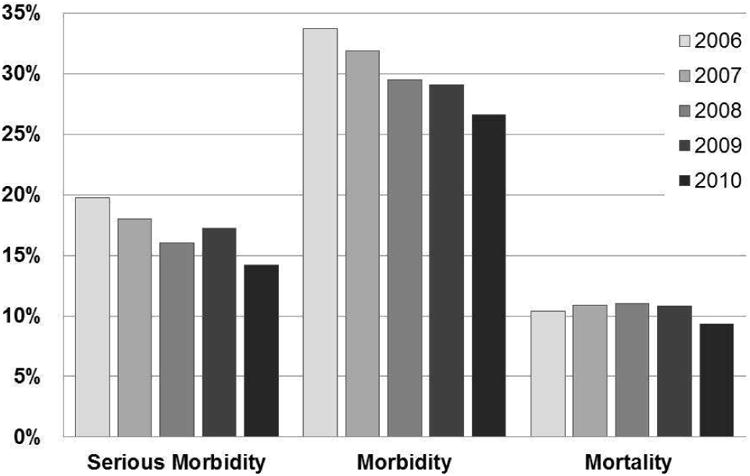
The prevalence of surgical intervention for DMa declined slightly over the time period, from 1.9%-1.6% of all procedures (P < 0.01). Among DMa patients, the most frequent operations performed were bowel resection, other gastrointestinal procedures, and multivisceral resections, these all showed small statistically significant decreases over time (P < 0.01). The rate of emergency operations also decreased (P < 0.01). In contrast, the rate of preoperative independent functional status rose, whereas the rate of preoperative weight loss and sepsis decreased (P < 0.01). Rates of 30-d morbidity (33.7 versus 26.6%), serious morbidity (19.8 versus 14.2%), and mortality (10.4 versus 9.3%) all decreased over the study period (P < 0.05). Multivariate analysis identified standard predictors (e.g., impaired functional status, preoperative weight loss, preoperative sepsis, and hypoalbuminemia) of worse 30-d M&M.
Thirty-day morbidity, serious morbidity, and mortality have decreased incrementally for patients with DMa undergoing surgical intervention, but surgical intervention remains prevalent. These data further highlight the importance of careful patient selection and goal-directed therapy in patients with incurable malignancy.
播散性恶性肿瘤(DMa)患者的手术发病率和死亡率(M&M)很高,一些人对手术的作用提出了质疑。因此,我们试图描述DMa患者M&M的时间趋势,假设手术干预仍将普遍存在。
我们查询了2006年至2010年美国外科医师学会国家外科质量改进计划。排除接受原发性肝脏手术的患者后,我们确定了21755例DMa患者。使用参数和/或非参数统计以及逻辑回归来评估M&M的时间趋势和预测因素。
在此期间,DMa手术干预的患病率略有下降,从所有手术的1.9%降至1.6%(P<0.01)。在DMa患者中,最常进行的手术是肠切除术、其他胃肠道手术和多脏器切除术,这些手术随着时间的推移均显示出统计学上的小幅显著下降(P<0.01)。急诊手术率也有所下降(P<0.01)。相比之下,术前独立功能状态的比率上升,而术前体重减轻和脓毒症的比率下降(P<0.01)。在研究期间,30天发病率(33.7%对26.6%)、严重发病率(19.8%对14.2%)和死亡率(10.4%对9.3%)均有所下降(P<0.05)。多变量分析确定了30天M&M较差的标准预测因素(如功能状态受损、术前体重减轻、术前脓毒症和低白蛋白血症)。
接受手术干预的DMa患者的30天发病率、严重发病率和死亡率逐渐下降,但手术干预仍然普遍。这些数据进一步强调了在无法治愈的恶性肿瘤患者中仔细选择患者和进行目标导向治疗的重要性。