Waweru Evelyn, Goodman Catherine, Kedenge Sarah, Tsofa Benjamin, Molyneux Sassy
Department of Public Health Research, Kenya Medical Research Institute-Wellcome Trust Research Programme, P.O. Box 230, 80108, Kilifi, Kenya,
Department for Global Health and Development, London School of Hygiene & Tropical Medicine, Keppel St., London, UK.
Health Policy Plan. 2016 Mar;31(2):137-47. doi: 10.1093/heapol/czv030. Epub 2015 Apr 28.
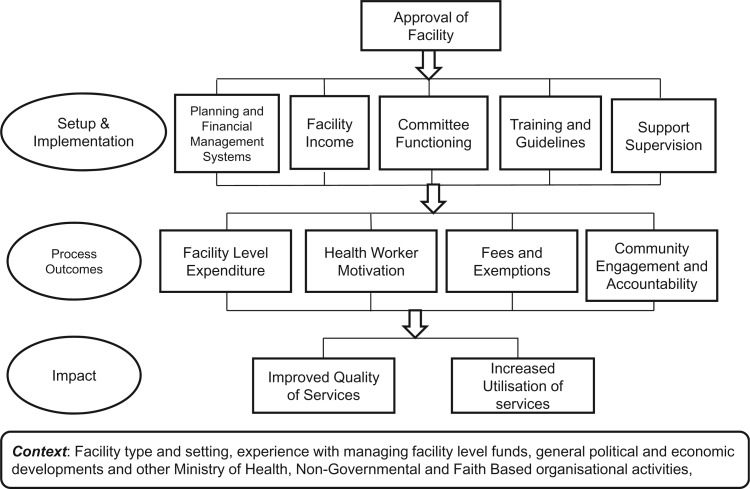
In many African countries, user fees have failed to achieve intended access and quality of care improvements. Subsequent user fee reduction or elimination policies have often been poorly planned, without alternative sources of income for facilities. We describe early implementation of an innovative national health financing intervention in Kenya; the health sector services fund (HSSF). In HSSF, central funds are credited directly into a facility's bank account quarterly, and facility funds are managed by health facility management committees (HFMCs) including community representatives. HSSF is therefore a finance mechanism with potential to increase access to funds for peripheral facilities, support user fee reduction and improve equity in access. We conducted a process evaluation of HSSF implementation based on a theory of change underpinning the intervention. Methods included interviews at national, district and facility levels, facility record reviews, a structured exit survey and a document review. We found impressive achievements: HSSF funds were reaching facilities; funds were being overseen and used in a way that strengthened transparency and community involvement; and health workers' motivation and patient satisfaction improved. Challenges or unintended outcomes included: complex and centralized accounting requirements undermining efficiency; interactions between HSSF and user fees leading to difficulties in accessing crucial user fee funds; and some relationship problems between key players. Although user fees charged had not increased, national reduction policies were still not being adhered to. Finance mechanisms can have a strong positive impact on peripheral facilities, and HFMCs can play a valuable role in managing facilities. Although fiduciary oversight is essential, mechanisms should allow for local decision-making and ensure that unmanageable paperwork is avoided. There are also limits to what can be achieved with relatively small funds in contexts of enormous need. Process evaluations tracking (un)intended consequences of interventions can contribute to regional financing and decentralization debates.
在许多非洲国家,使用者付费未能实现预期的医疗服务可及性提升和质量改善。随后的使用者付费减免或取消政策往往规划不善,且医疗机构没有其他收入来源。我们描述了肯尼亚一项创新性国家卫生筹资干预措施——卫生部门服务基金(HSSF)的早期实施情况。在HSSF模式下,中央资金每季度直接存入医疗机构的银行账户,医疗机构资金由包括社区代表在内的卫生机构管理委员会(HFMCs)管理。因此,HSSF是一种有潜力增加周边医疗机构资金可及性、支持减免使用者付费并改善医疗服务可及性公平性的筹资机制。我们基于该干预措施的变革理论对HSSF的实施进行了过程评估。方法包括在国家、地区和医疗机构层面进行访谈、审查医疗机构记录、开展结构化的出院调查以及文件审查。我们发现了令人瞩目的成果:HSSF资金到达了各医疗机构;资金的监督和使用方式增强了透明度并提高了社区参与度;卫生工作者的积极性和患者满意度得到了提升。挑战或意外结果包括:复杂且集中的会计要求降低了效率;HSSF与使用者付费之间的相互作用导致获取关键的使用者付费资金存在困难;以及关键参与者之间存在一些关系问题。尽管收取的使用者付费没有增加,但国家的减免政策仍未得到遵守。筹资机制可以对周边医疗机构产生强大的积极影响,并且HFMCs在管理医疗机构方面可以发挥重要作用。尽管信托监督至关重要,但机制应允许地方决策并确保避免难以管理的文书工作。在需求巨大的情况下,相对较少的资金所能取得的成果也存在局限性。跟踪干预措施(非)预期后果的过程评估有助于区域筹资和权力下放的辩论。