Shalapour Shabnam, Font-Burgada Joan, Di Caro Giuseppe, Zhong Zhenyu, Sanchez-Lopez Elsa, Dhar Debanjan, Willimsky Gerald, Ammirante Massimo, Strasner Amy, Hansel Donna E, Jamieson Christina, Kane Christopher J, Klatte Tobias, Birner Peter, Kenner Lukas, Karin Michael
1] Laboratory of Gene Regulation and Signal Transduction, Department of Pharmacology, School of Medicine, University of California San Diego (UCSD), 9500 Gilman Drive, San Diego, California 92093, USA [2] Department of Pathology, School of Medicine, University of California San Diego, 9500 Gilman Drive, San Diego, California 92093, USA.
Institute of Immunology, Charité Campus Buch, 13125 Berlin, Germany.
Nature. 2015 May 7;521(7550):94-8. doi: 10.1038/nature14395. Epub 2015 Apr 29.
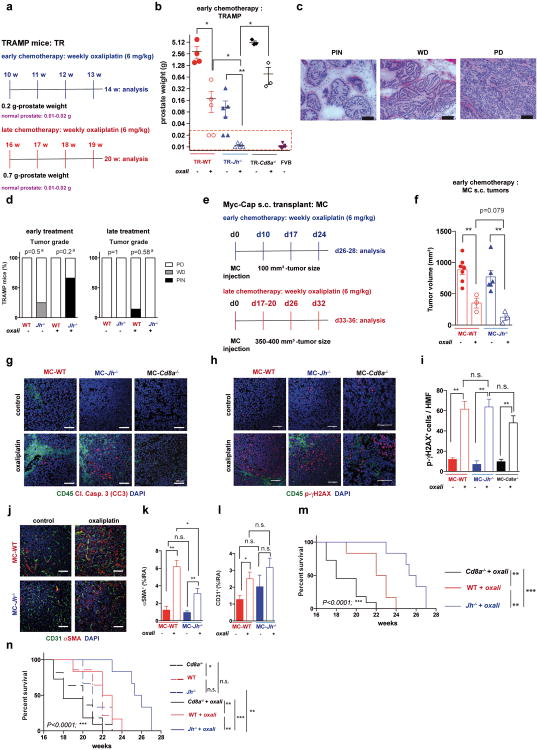
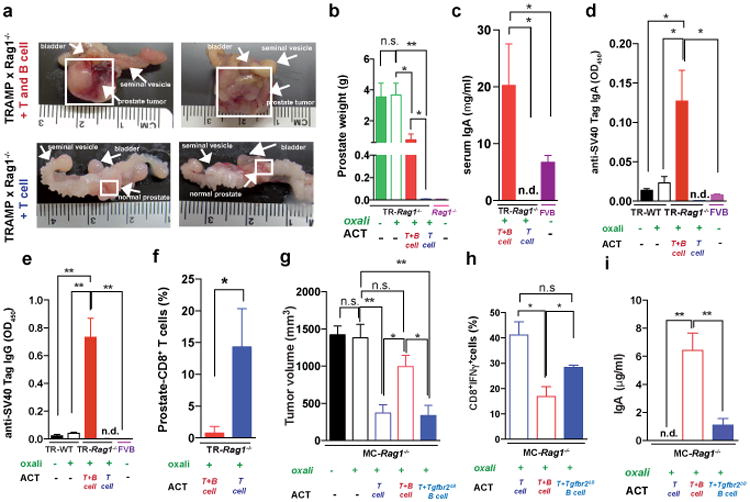
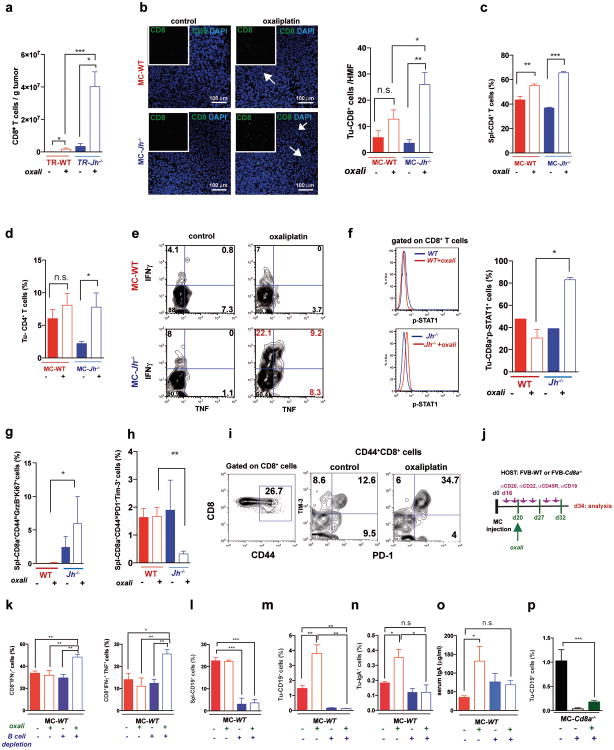
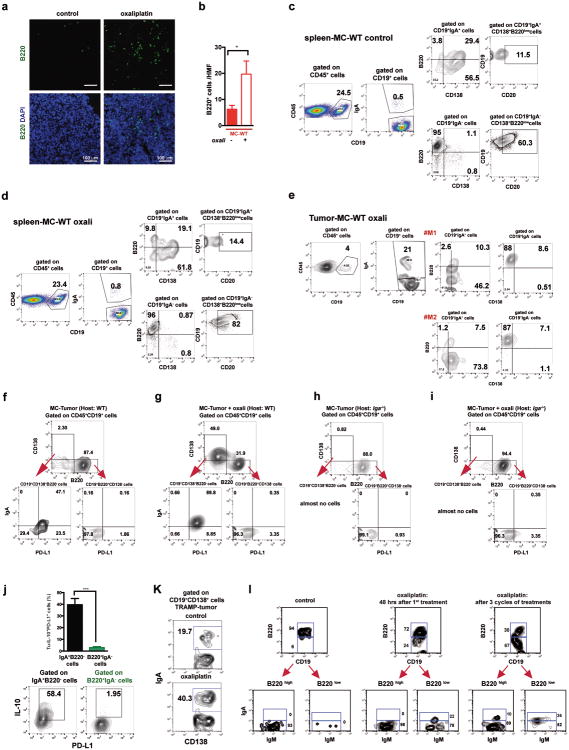
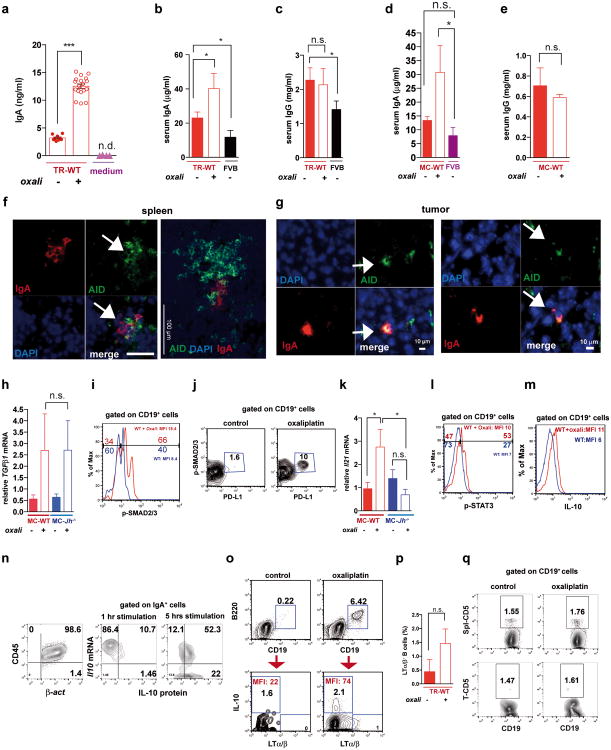
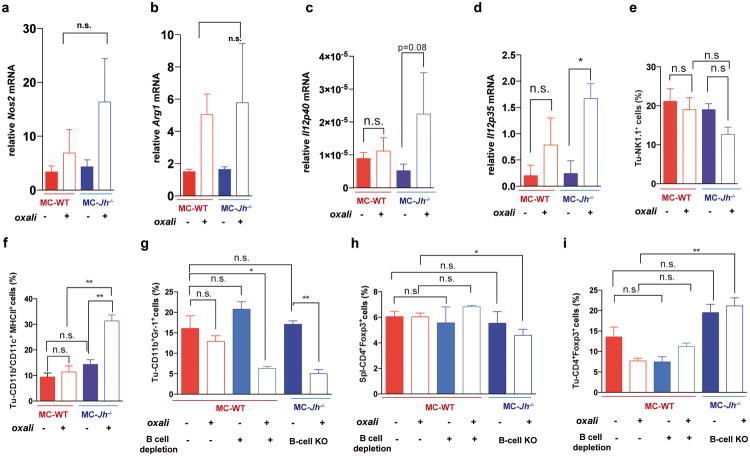
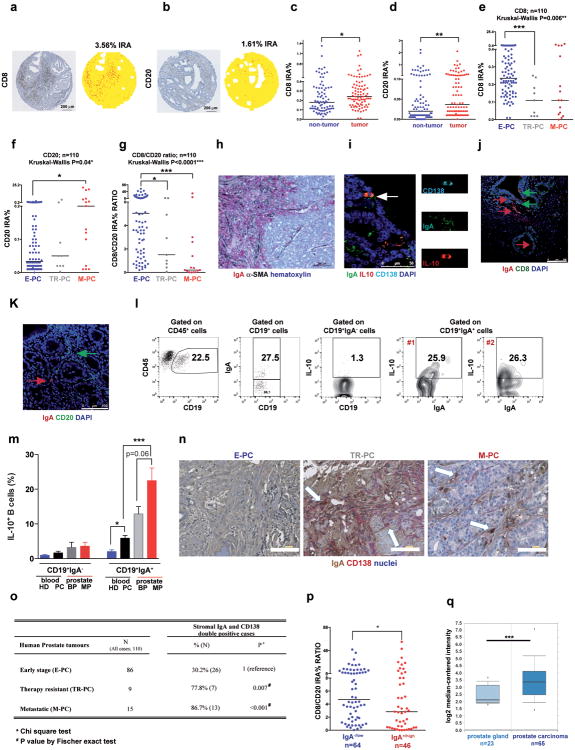
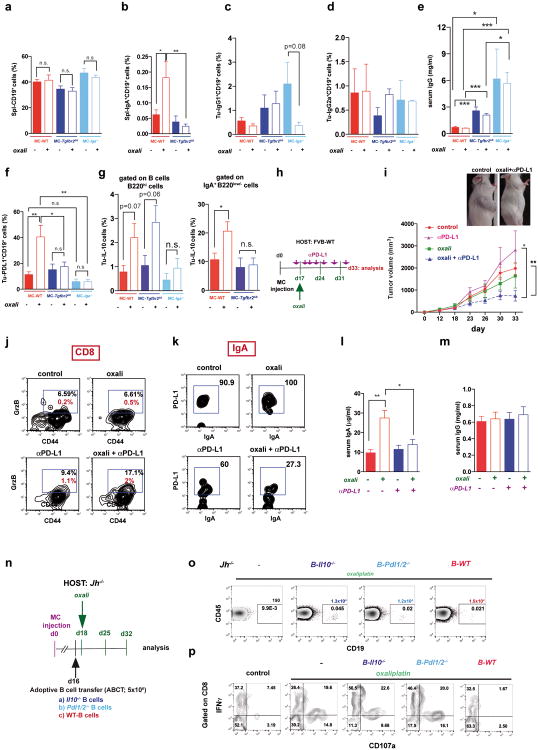
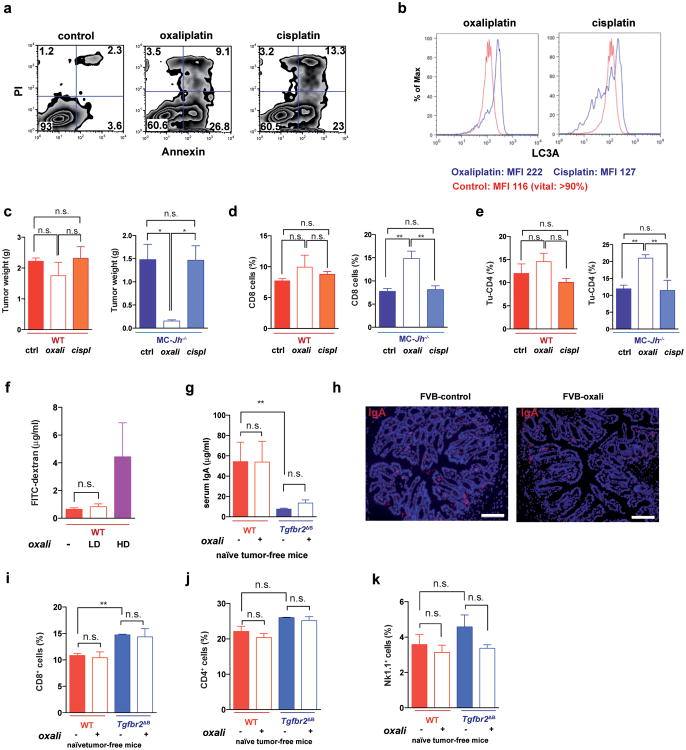
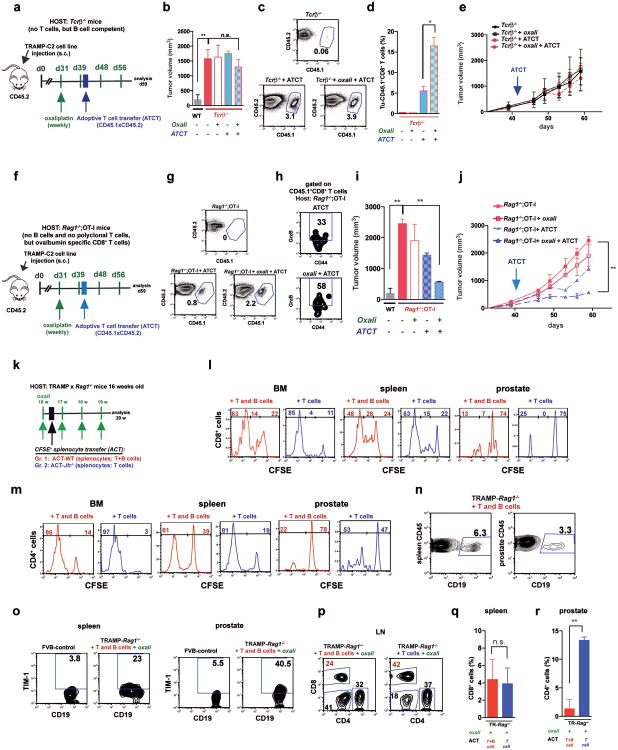
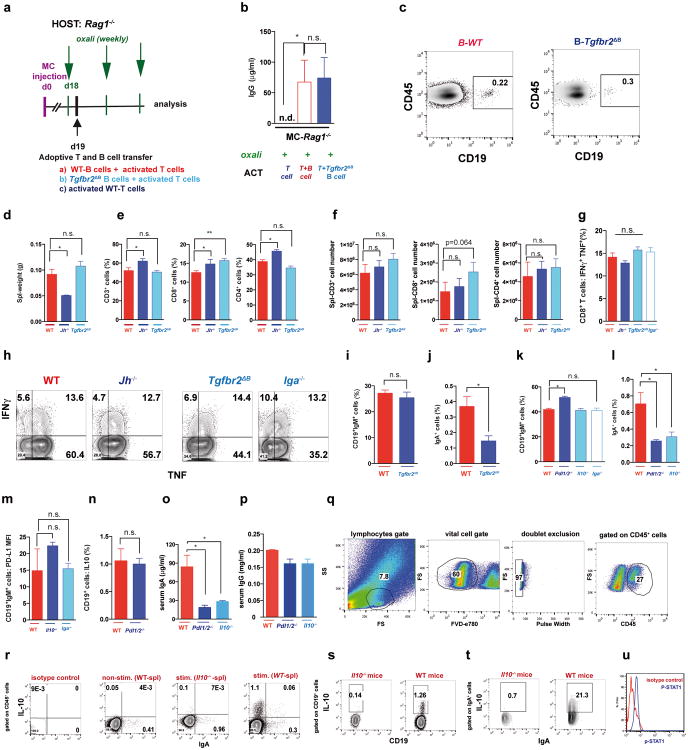
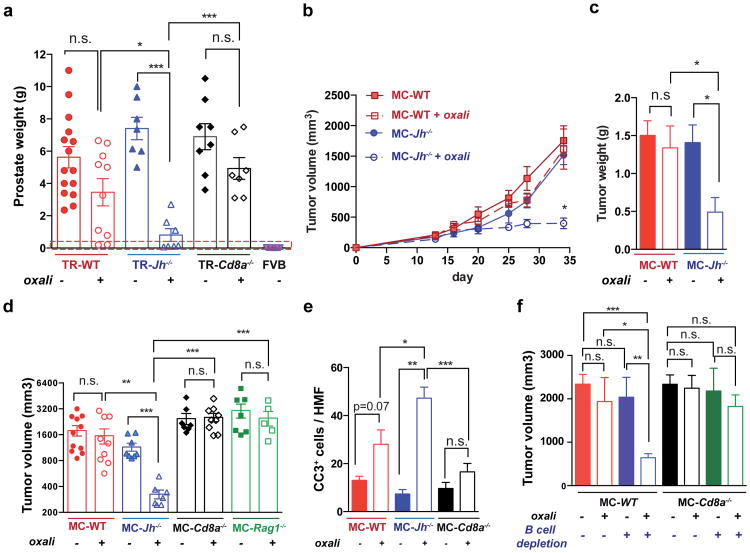
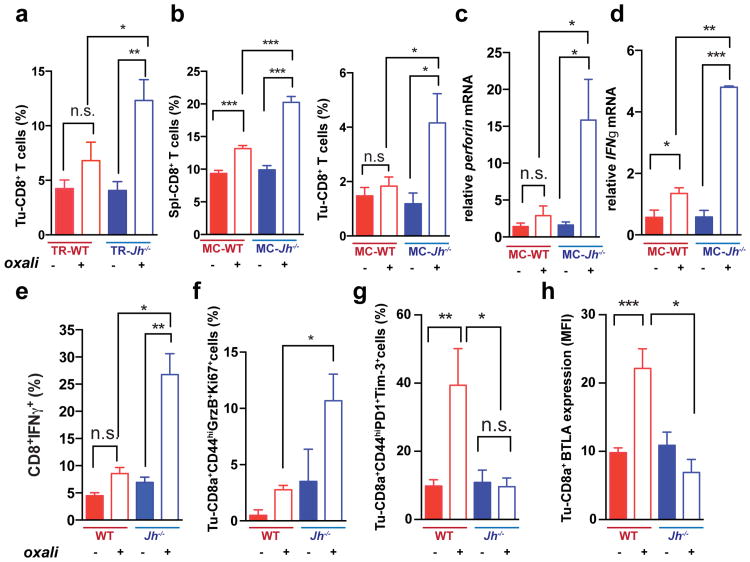
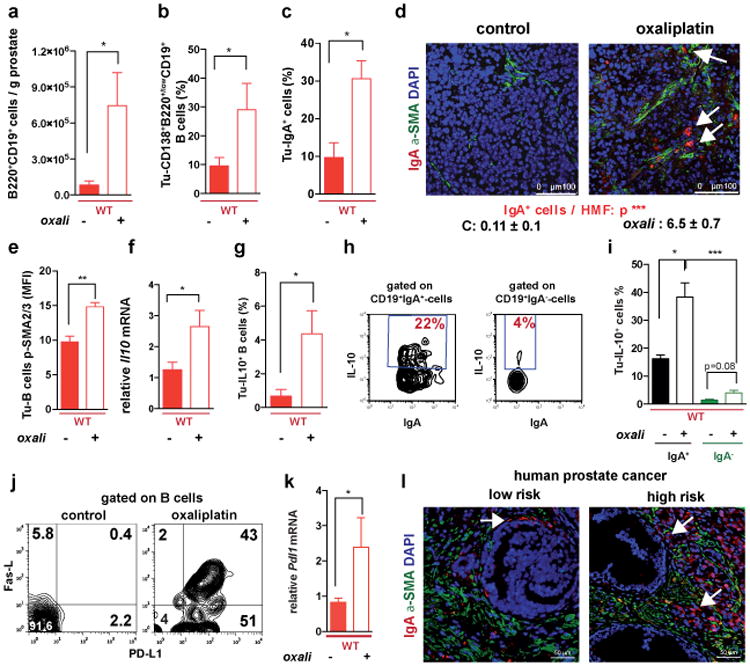
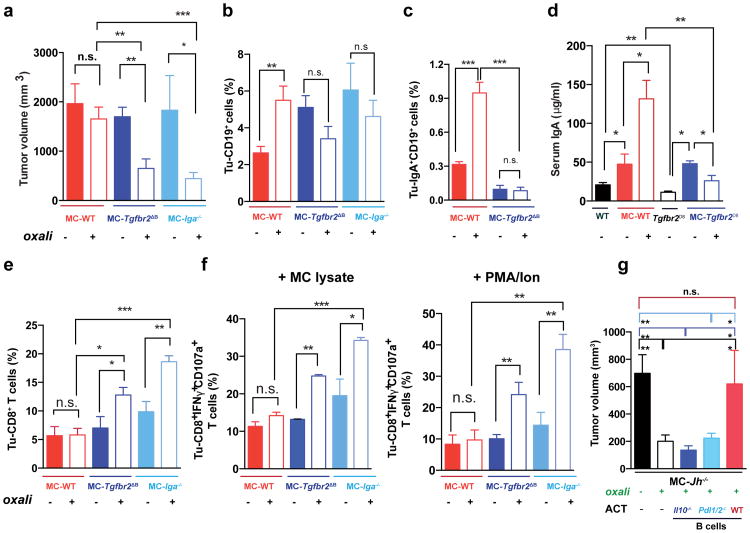
Cancer-associated genetic alterations induce expression of tumour antigens that can activate CD8(+) cytotoxic T cells (CTLs), but the microenvironment of established tumours promotes immune tolerance through poorly understood mechanisms. Recently developed therapeutics that overcome tolerogenic mechanisms activate tumour-directed CTLs and are effective in some human cancers. Immune mechanisms also affect treatment outcome, and certain chemotherapeutic drugs stimulate cancer-specific immune responses by inducing immunogenic cell death and other effector mechanisms. Our previous studies revealed that B cells recruited by the chemokine CXCL13 into prostate cancer tumours promote the progression of castrate-resistant prostate cancer by producing lymphotoxin, which activates an IκB kinase α (IKKα)-BMI1 module in prostate cancer stem cells. Because castrate-resistant prostate cancer is refractory to most therapies, we examined B cell involvement in the acquisition of chemotherapy resistance. Here we focus on oxaliplatin, an immunogenic chemotherapeutic agent that is effective in aggressive prostate cancer. We show that mouse B cells modulate the response to low-dose oxaliplatin, which promotes tumour-directed CTL activation by inducing immunogenic cell death. Three different mouse prostate cancer models were refractory to oxaliplatin unless genetically or pharmacologically depleted of B cells. The crucial immunosuppressive B cells are plasmocytes that express IgA, interleukin (IL)-10 and programmed death ligand 1 (PD-L1), the appearance of which depends on TGFβ receptor signalling. Elimination of these cells, which also infiltrate human-therapy-resistant prostate cancer, allows CTL-dependent eradication of oxaliplatin-treated tumours.
癌症相关的基因改变会诱导肿瘤抗原的表达,这些抗原可激活CD8(+)细胞毒性T细胞(CTL),但已形成肿瘤的微环境会通过尚不明确的机制促进免疫耐受。最近开发的克服致耐受机制的疗法可激活肿瘤定向CTL,并在某些人类癌症中有效。免疫机制也会影响治疗结果,某些化疗药物通过诱导免疫原性细胞死亡和其他效应机制来刺激癌症特异性免疫反应。我们之前的研究表明,趋化因子CXCL13招募到前列腺癌肿瘤中的B细胞通过产生淋巴毒素促进去势抵抗性前列腺癌的进展,淋巴毒素可激活前列腺癌干细胞中的IκB激酶α(IKKα)-BMI1模块。由于去势抵抗性前列腺癌对大多数疗法均具有抗性,我们研究了B细胞在获得化疗抗性中的作用。在这里,我们重点关注奥沙利铂,这是一种对侵袭性前列腺癌有效的免疫原性化疗药物。我们发现小鼠B细胞可调节对低剂量奥沙利铂的反应,奥沙利铂通过诱导免疫原性细胞死亡促进肿瘤定向CTL的激活。三种不同的小鼠前列腺癌模型对奥沙利铂均具有抗性,除非通过基因或药物手段清除B细胞。关键的免疫抑制性B细胞是表达IgA、白细胞介素(IL)-10和程序性死亡配体1(PD-L1)的浆细胞,其出现依赖于TGFβ受体信号传导。清除这些也浸润到对人类治疗有抗性的前列腺癌中的细胞,可使CTL依赖的奥沙利铂治疗肿瘤得以根除。